📋 Key Information Summary
- Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia, affecting approximately 380,000 Australians, with prevalence increasing sharply with age and expected to double by 2050.
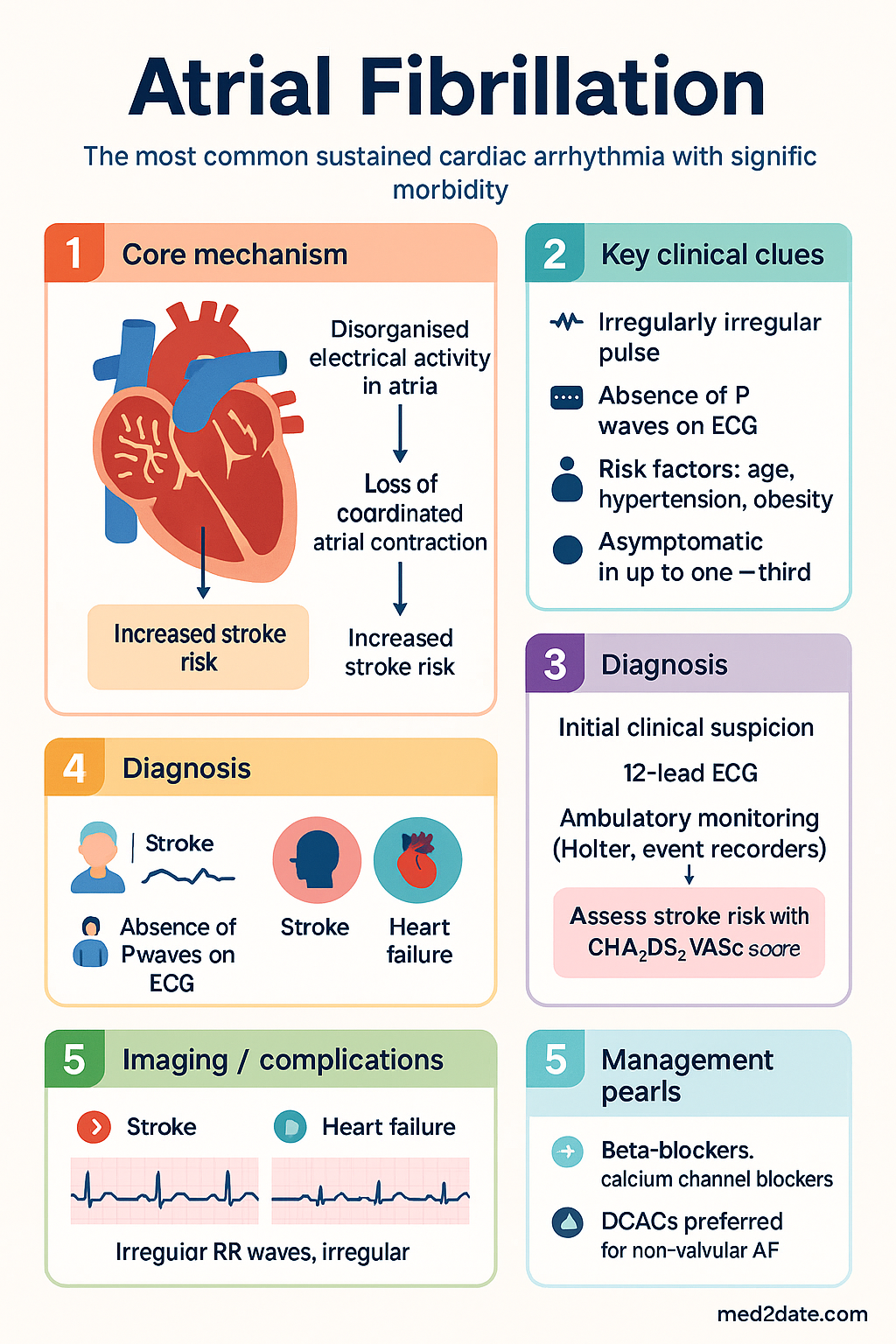
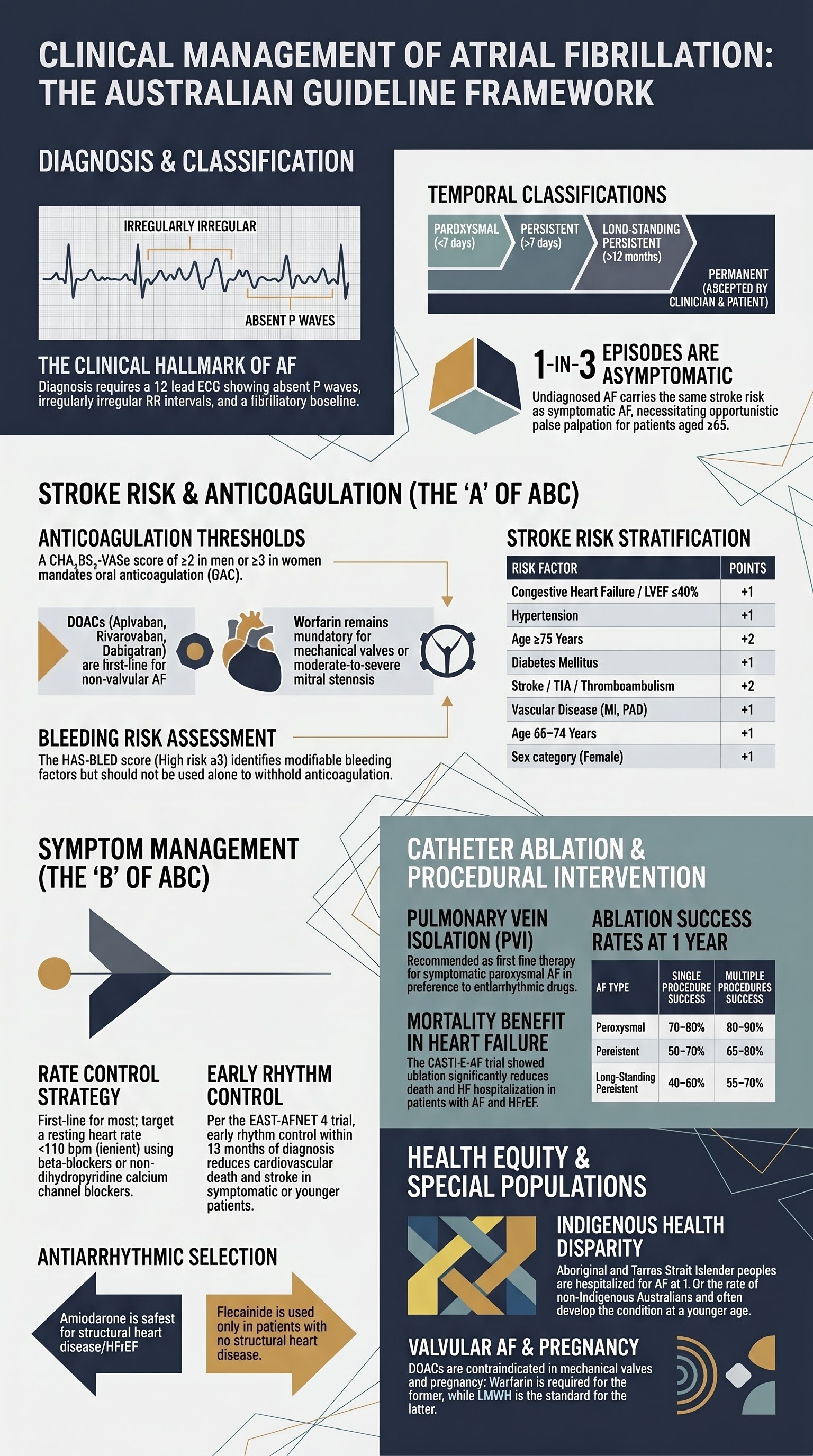
- Classification: Paroxysmal (self-terminating within 7 days), persistent (sustained >7 days or requiring cardioversion), long-standing persistent (>12 months), and permanent (accepted by patient and clinician).
- Diagnosis requires a 12-lead ECG showing absence of distinct P waves, irregularly irregular RR intervals, and fibrillatory baseline. Ambulatory monitoring (Holter, event recorders, implantable loop recorders) captures paroxysmal episodes.
- Stroke risk stratification uses CHA₂DS₂-VASc. Score ≥2 in men or ≥3 in women mandates oral anticoagulation (OAC). Score 1 in men warrants individualised consideration.
- DOACs (apixaban, rivaroxaban, dabigatran, edoxaban) are first-line over warfarin for non-valvular AF, with superior safety profiles and no routine INR monitoring required.
- Warfarin remains essential for mechanical heart valves and moderate-to-severe mitral stenosis (valvular AF). Target INR 2.0–3.0 for most indications.
- Rate control is first-line strategy for most patients. Target resting heart rate <110 bpm (lenient) or <80 bpm (strict). First-line agents include beta-blockers and non-dihydropyridine calcium channel blockers.
- Rhythm control is preferred in younger, symptomatic patients, first detected AF, AF secondary to treatable cause, or when rate control fails. Options include antiarrhythmic drugs, cardioversion, and catheter ablation.
- Catheter ablation (pulmonary vein isolation) is superior to antiarrhythmic drugs for maintaining sinus rhythm and is recommended as first-line in selected symptomatic patients, including those with HFrEF.
- CHA₂DS₂-VASc components: CHF (+1), Hypertension (+1), Age ≥75 (+2), Diabetes (+1), Stroke/TIA/TE (+2), Vascular disease (+1), Age 65–74 (+1), Sex category female (+1).
- Aboriginal and Torres Strait Islander peoples have significantly higher AF prevalence, younger age of onset, higher stroke rates, and lower anticoagulant use — culturally safe, community-based approaches are essential.
- All anticoagulated patients require regular review of adherence, bleeding risk (HAS-BLED), renal function, and drug interactions. Reassess at least annually or with any clinical change.
Introduction & Australian Epidemiology
Atrial fibrillation (AF) is characterised by disorganised electrical activity in the atria, resulting in an irregularly irregular ventricular response and loss of coordinated atrial contraction. It is the most common sustained cardiac arrhythmia worldwide and carries significant morbidity through stroke, heart failure, reduced quality of life, and increased mortality.
In Australia, an estimated 380,000 people live with AF, though the true burden is likely higher due to undiagnosed paroxysmal episodes. AF prevalence increases with age: it affects approximately 1% of those under 60 years but rises to 8–10% in those aged 80 years and older. The AIHW reports AF-related hospitalisations exceeded 90,000 admissions annually, making it a leading cardiovascular cause of hospital presentation.
AF carries a five-fold increase in stroke risk, and AF-related strokes tend to be more severe with higher mortality and disability. The total economic cost of AF in Australia is estimated at over .5 billion annually, including direct healthcare costs and lost productivity.
Risk factors for AF include advancing age, hypertension, obesity, obstructive sleep apnoea, valvular heart disease, heart failure, diabetes, excessive alcohol intake, and hyperthyroidism. Modifiable risk factors should be aggressively addressed as part of a holistic AF management strategy, consistent with the AF Better Care (ABC) pathway endorsed by international guidelines.
Classification & Diagnosis
Classification of Atrial Fibrillation
AF is classified based on temporal pattern and duration. Accurate classification guides management decisions regarding rate vs rhythm control strategy and anticoagulation approach.
ECG Diagnosis
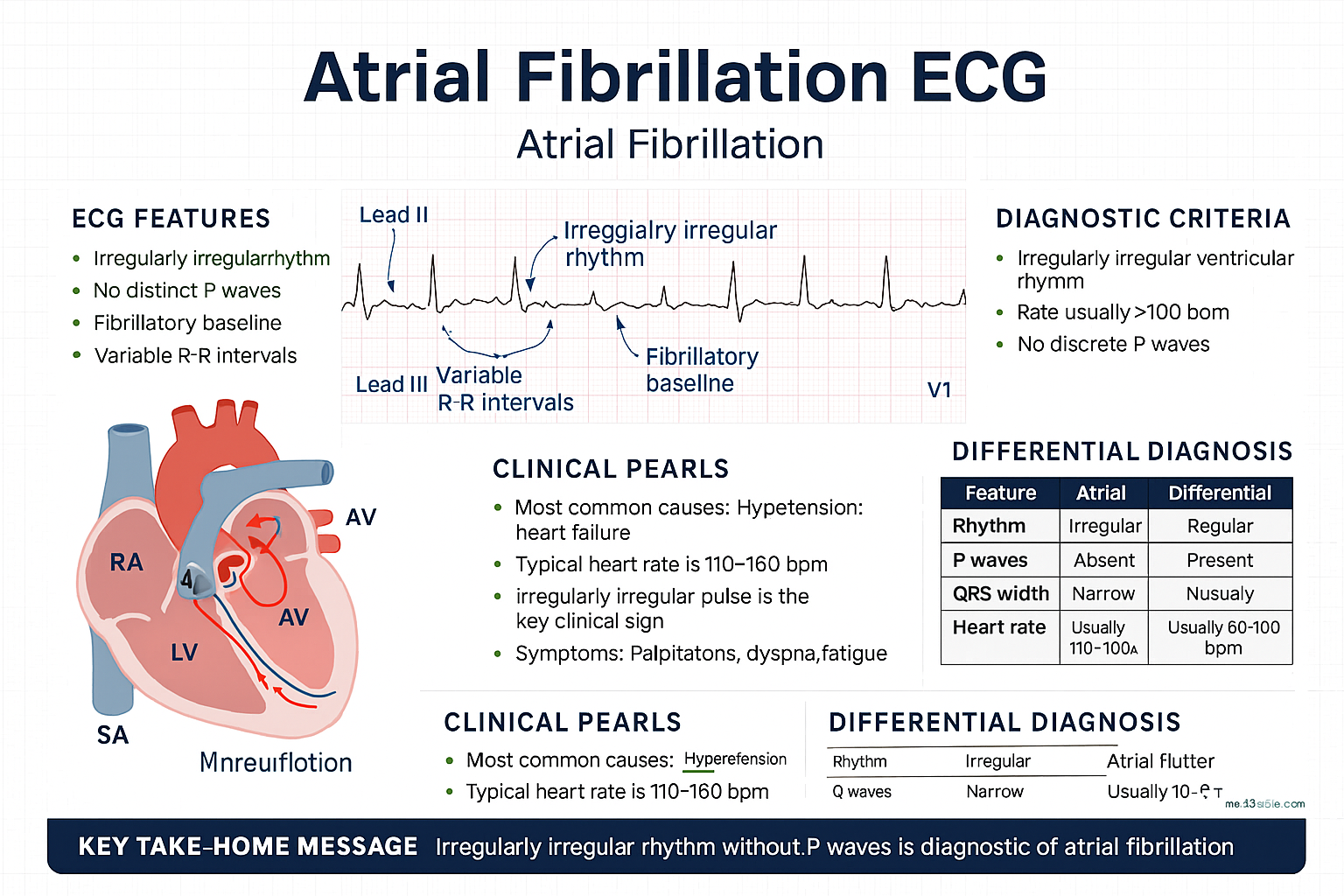
The hallmark 12-lead ECG findings of AF are:
- Absent P waves — replaced by irregular, low-amplitude fibrillatory (f) waves, best seen in leads V1, II, III, and aVF
- Irregularly irregular RR intervals — the most readily identifiable feature at the bedside
- Narrow QRS complex (unless aberrant conduction or pre-existing bundle branch block)
- Absence of an isoelectric baseline between QRS complexes
- Variable ventricular rate — typically 100–160 bpm if untreated; may be slow (<60 bpm) suggesting concomitant AV node disease or rate-controlling medication effect
Ambulatory Monitoring
Since paroxysmal AF is often asymptomatic and may not be captured on a standard ECG, ambulatory monitoring plays a critical role in diagnosis:
| Modality | Duration | Indication | Australian Availability |
|---|---|---|---|
| 24–48-hour Holter monitor | 1–2 days | Symptoms occurring daily | Widely available (MBS Item 11706) |
| Extended Holter / 7-day patch | 7–14 days | Intermittent symptoms (weekly) | Available in most cardiology practices |
| Event recorder (external) | Up to 30 days | Infrequent symptoms (monthly) | Available; MBS Item 11707 |
| Smartwatch / consumer devices | Continuous | Screening; symptom correlation | Not MBS-funded; clinical validation advised |
| Implantable loop recorder (ILR) | Up to 3 years | Cryptogenic stroke workup; infrequent paroxysmal AF | Available; requires procedural facility (MBS Item 38280) |
Population Screening
The National Heart Foundation of Australia (NHFA) and Cardiac Society of Australia and New Zealand (CSANZ) recommend opportunistic pulse palpation during routine clinical encounters for patients aged ≥65 years. An irregular pulse should prompt a 12-lead ECG for confirmation. Systematic screening with single-lead ECG or automated devices may be considered in high-risk populations, including post-stroke patients and those aged ≥75 with additional risk factors.
Smartwatch-based photoplethysmography (PPG) detection algorithms show high specificity but moderate sensitivity. Any positive result from a consumer device requires confirmatory ECG before initiating anticoagulation.
Stroke Risk & Anticoagulation
CHA₂DS₂-VASc Score
The CHA₂DS₂-VASc score is the recommended tool for stroke risk stratification in non-valvular AF. It builds upon the earlier CHADS₂ score with additional risk factors, improving identification of truly low-risk patients.
| Risk Factor | Points |
|---|---|
| C — Congestive heart failure (or LVEF ≤40%) | +1 |
| H — Hypertension | +1 |
| A₂ — Age ≥75 years | +2 |
| D — Diabetes mellitus | +1 |
| S₂ — Stroke/TIA/thromboembolism history | +2 |
| V — Vascular disease (MI, PAD, aortic plaque) | +1 |
| A — Age 65–74 years | +1 |
| Sc — Sex category (female) | +1 |
Anticoagulation Thresholds
Anticoagulant Selection
Direct oral anticoagulants (DOACs) are recommended as first-line over warfarin for non-valvular AF based on the pivotal RE-LY, ROCKET-AF, ARISTOTLE, and ENGAGE AF-TIMI 48 trials, and endorsed by NHFA/CSANZ, ESC, and AHA/ACC guidelines.
Bleeding Risk — HAS-BLED Score
The HAS-BLED score identifies modifiable bleeding risk factors and promotes their correction. It should not be used to withhold anticoagulation but rather to trigger regular clinical review and correction of reversible risk factors.
| Letter | Risk Factor | Points |
|---|---|---|
| H | Hypertension (uncontrolled, SBP >160 mmHg) | +1 |
| A | Abnormal renal or liver function (1 point each) | +1 or +2 |
| S | Stroke history | +1 |
| B | Bleeding history or predisposition | +1 |
| L | Labile INR (TTR <60%, only if on warfarin) | +1 |
| E | Elderly (>65 years) | +1 |
| D | Drugs (antiplatelets, NSAIDs) or alcohol excess | +1 or +2 |
HAS-BLED ≥3: High bleeding risk — not a contraindication to anticoagulation, but mandates closer monitoring, correction of modifiable factors (control BP, discontinue concomitant antiplatelet/NSAID, address alcohol use), and regular clinical review.
Left Atrial Appendage Occlusion
For patients with AF who have genuine contraindications to long-term anticoagulation (e.g. life-threatening haemorrhage, recurrent major bleeding despite optimal therapy), left atrial appendage occlusion (LAAO) with devices such as the Watchman™ may be considered. This requires referral to a specialist centre with procedural expertise. It is available in select Australian tertiary centres and is funded through hospital-based programmes in some states.
Rate Control Strategies
Rate control is the recommended initial strategy for most patients with AF, as demonstrated by the AFFIRM, RACE, and AF-CHF trials which showed no mortality benefit of rhythm control over rate control. The target heart rate remains controversial, but the RACE II trial supports a lenient target (resting HR <110 bpm) as non-inferior to strict control (<80 bpm) for most patients. A stricter target may be considered if symptoms persist at lenient targets.
First-Line Rate Control Agents
Rate Control Quick Reference
AV Node Ablation + Permanent Pacing
When pharmacological rate control is inadequate or poorly tolerated despite optimal combination therapy, AV node ablation with permanent pacemaker implantation ("ablate and pace") is an effective last-resort strategy. This creates complete heart block with reliable ventricular rate control via pacing.
- Requires permanent pacemaker — typically DDDR or VVIR mode
- Results in pacemaker dependency — irreversible procedure
- Consider CRT-pacing (CRT-P) if LVEF <35–50% to reduce RV pacing-induced dyssynchrony
- Improves quality of life in 80–90% of appropriately selected patients
- Anticoagulation still required — patient remains in AF
Rhythm Control Strategies
Rhythm control aims to restore and maintain sinus rhythm. While earlier trials (AFFIRM, RACE) showed no mortality advantage over rate control, the EAST-AFNET 4 trial (2020) demonstrated that early rhythm control within 12 months of AF diagnosis significantly reduced cardiovascular outcomes (composite of stroke, HF, acute coronary syndrome, cardiovascular death), particularly in patients with low AF burden and fewer comorbidities.
When to Choose Rhythm Control
- Symptomatic AF despite adequate rate control
- First-detected or recently diagnosed AF (<12 months) with CV risk factors (EAST-AFNET 4)
- Younger patients where AF progression is a concern
- AF precipitated by a reversible cause (e.g. hyperthyroidism, post-operative, alcohol)
- Patient preference after shared decision-making
- Tachycardia-mediated cardiomyopathy despite rate control
- Intolerance to rate-controlling agents
Antiarrhythmic Drug Selection
Antiarrhythmic drugs for rhythm control in AF are classified per the Vaughan-Williams system. The choice depends on underlying structural heart disease, LVEF, and comorbidities.
Antiarrhythmic Drug Selection by Heart Disease
| Clinical Scenario | First-Line | Second-Line | Avoid |
|---|---|---|---|
| No structural heart disease | Flecainide or propafenone | Sotalol, dronedarone, or catheter ablation | — |
| Coronary artery disease | Sotalol or dronedarone | Amiodarone, catheter ablation | Flecainide, propafenone |
| HFrEF (LVEF ≤40%) | Amiodarone or catheter ablation | Dronedarone (mild HF only) | Flecainide, propafenone, sotalol |
| Hypertrophic cardiomyopathy | Amiodarone | Dronedarone, catheter ablation | Flecainide, propafenone |
Pharmacological Cardioversion
Pharmacological cardioversion is most effective within 7 days of AF onset. Options include:
- Flecainide PO 200–300 mg stat (if no structural heart disease) — conversion rate ~50–70% within 3–6 hours
- Amiodarone IV — slower onset but safe in structural heart disease; may convert over 24 hours
- Vernakalant IV (Kynapid®) — approved in Australia for rapid conversion of recent-onset AF (<7 days); MBS access limited to hospital use
- Flecainide + oral beta-blocker combo — "pill-in-the-pocket" approach for patients with infrequent, well-tolerated paroxysmal AF
Electrical Cardioversion
Synchronised DC cardioversion is performed under procedural sedation (propofol or midazolam + fentanyl) with continuous monitoring. Biphasic defibrillators are standard, with initial energy of 120–200 J biphasic. Success rates exceed 90% for recent-onset AF. Paddles should be placed in anterolateral or anteroposterior positions. All patients require the same anticoagulation strategy as for pharmacological cardioversion.
Catheter Ablation
Pulmonary Vein Isolation (PVI)
Catheter ablation for AF is centred on pulmonary vein isolation (PVI), which electrically isolates the pulmonary veins from the left atrium to eliminate the triggers and substrate for AF. This is typically achieved using either radiofrequency (RF) ablation with point-by-point lesion sets or cryoballoon ablation which achieves single-shot PVI. Pulsed field ablation (PFA) is an emerging technology with tissue selectivity, reducing collateral damage to oesophagus and phrenic nerve.
Indications for Catheter Ablation
- Paroxysmal AF: Recommended as first-line or after failure of one antiarrhythmic drug. Single-procedure success rate 70–80% at 1 year
- Persistent AF: Recommended after failure of antiarrhythmic drugs. May require substrate modification beyond PVI. Success rate 50–70% at 1 year
- Long-standing persistent AF: Considered in selected symptomatic patients. Lower success rate (40–60%); may require multiple procedures
- AF with HFrEF: CASTLE-AF trial demonstrated mortality and HF hospitalisation benefit of ablation vs medical therapy. Recommended when AF is contributing to ventricular dysfunction
- Patient preference: Shared decision-making; some patients prefer ablation over lifelong antiarrhythmic drug therapy
Procedural Success Rates
| AF Type | Single Procedure Success (1 year) | Multiple Procedures Success (1 year) | 5-Year Freedom from AF |
|---|---|---|---|
| Paroxysmal | 70–80% | 80–90% | 50–70% |
| Persistent | 50–70% | 65–80% | 40–60% |
| Long-standing persistent | 40–60% | 55–70% | 30–50% |
Complications
Catheter ablation for AF carries a recognised complication profile. Overall major complication rate is 2–4% at experienced centres:
- Cardiac tamponade (1–2%) — most significant acute emergency; requires pericardiocentesis
- Pulmonary vein stenosis (<1%) — reduced with modern wide-antral isolation techniques
- Atrio-oesophageal fistula (0.01–0.25%) — rare but highly lethal; presents days to weeks post-procedure with fever, neurological symptoms, mediastinitis. High index of suspicion required
- Phrenic nerve injury (0.5–2%) — more common with cryoballoon; usually transient
- Stroke/TIA (0.5–1%) — minimised with anticoagulation and heparinisation during procedure
- Vascular access complications (2–4%) — haematoma, pseudoaneurysm, AV fistula
- Death (<0.1%) — extremely rare
Repeat Procedures
A significant proportion of patients require repeat ablation procedures. Pulmonary vein reconnection is the most common mechanism of AF recurrence. For paroxysmal AF, a second procedure is needed in 20–30% of patients. For persistent AF, 30–50% may require a second procedure. A third procedure is uncommon and should prompt re-evaluation of the rhythm control strategy. A blanking period of 3 months post-ablation should be observed before assessing treatment failure, as early recurrences (up to 50%) may resolve with healing and antiarrhythmic drug therapy during this period.
Australian Access
Catheter ablation for AF is available at major metropolitan centres across all Australian states and territories. Waiting times in the public system can be 3–12 months depending on the centre. Private health insurance typically covers the procedure with minimal out-of-pocket costs at participating hospitals. Regional and remote patients may need to travel for the procedure, with post-operative follow-up coordinated with local cardiologists. MBS Item 38258 covers catheter ablation of arrhythmogenic substrate.
Special Populations
AF with HFrEF
Valvular AF
Post-Operative AF
Athlete's Heart & AF
Renal Impairment
Pregnancy
Investigations
A structured diagnostic workup is essential for every patient presenting with AF. Investigations should identify reversible causes, assess cardiac structure and function, quantify stroke and bleeding risk, and guide management strategy.
Monitoring
Anticoagulation Monitoring
Warfarin-Specific Monitoring
- INR target: 2.0–3.0 (2.5–3.5 for mechanical mitral valve)
- INR frequency: weekly until stable (3 consecutive INRs in range), then every 2–4 weeks
- Time in therapeutic range (TTR): aim >70% (Rosendaal method). If TTR consistently <65%, consider switching to DOAC
- Patient self-monitoring (home INR testing) is supported and improves TTR in motivated patients
- Significant drug interactions: antibiotics (metronidazole, fluconazole, macrolides), amiodarone (reduce warfarin dose by 30–50%), anticonvulsants, St John's wort
Antiarrhythmic Drug Monitoring
| Drug | Monitoring Required | Frequency |
|---|---|---|
| Amiodarone | TFTs, LFTs, CXR, ophthalmology review | TFTs/LFTs: 6-monthly. CXR: annual. Ophthalmology: annual |
| Sotalol | ECG (QTc), renal function, electrolytes | ECG: after initiation, dose change, and at steady state. Renal: 6-monthly |
| Flecainide | ECG (QRS duration), drug level if renal impairment | ECG: after initiation and annually |
| Dronedarone | ECG (QTc), LFTs, renal function | LFTs: baseline, then periodically. ECG: after initiation |
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of atrial fibrillation and its complications. Data from the AIHW and the Busselton Health Study demonstrate that Indigenous Australians develop AF at a younger age, have higher rates of comorbid conditions (rheumatic heart disease, diabetes, chronic kidney disease, obesity), and experience significantly higher rates of AF-related stroke and cardiovascular mortality compared to non-Indigenous Australians.
Despite the higher disease burden, studies consistently demonstrate lower rates of anticoagulant prescription in Indigenous AF patients. This "treatment gap" reflects systemic barriers including access to specialist care, medication affordability (particularly in remote communities), health literacy, cultural safety of health services, and the complexity of medication regimens.
AF Better Care (ABC) Pathway — Holistic Management
The AF Better Care (ABC) pathway, endorsed by the ESC and NHFA/CSANZ, provides a structured approach to integrated AF management. It has been shown to reduce stroke, major bleeding, cardiovascular mortality, and all-cause mortality when consistently applied.
📚 References
- 1. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2021;42(5):373-498.
- 2. Brieger D, Amerena J, Attia J, et al. National Heart Foundation of Australia and the Cardiac Society of Australia and New Zealand: Australian Clinical Guidelines for the Diagnosis and Management of Atrial Fibrillation 2018. Heart Lung Circ. 2018;27(10):1209-1266.
- 3. Kirchhof P, Camm AJ, Goette A, et al. Early rhythm-control therapy in patients with atrial fibrillation. N Engl J Med. 2020;383(14):1305-1316. (EAST-AFNET 4 trial)
- 4. Marrouche NF, Brachmann J, Andresen D, et al. Catheter ablation for atrial fibrillation with heart failure. N Engl J Med. 2018;378(5):417-427. (CASTLE-AF trial)
- 5. Van Gelder IC, Groenveld HF, Crijns HJ, et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010;362(15):1363-1373. (RACE II trial)
- 6. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365(11):981-992. (ARISTOTLE trial)
- 7. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361(12):1139-1151. (RE-LY trial)
- 8. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365(10):883-891. (ROCKET-AF trial)
- 9. Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369(22):2093-2104. (ENGAGE AF-TIMI 48 trial)
- 10. Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347(23):1825-1833. (AFFIRM trial)
- 11. Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the Euro Heart Survey on Atrial Fibrillation. Chest. 2010;137(2):263-272.
- 12. Australian Institute of Health and Welfare (AIHW). Atrial fibrillation in Australia. Cat. no. CVD 87. Canberra: AIHW; 2022.
- 13. National Heart Foundation of Australia. Guidelines for the management of absolute cardiovascular disease risk. Melbourne: NHF; 2012 (updated 2023).
- 14. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. Cat. no. CDK 10. Canberra: AIHW; 2023.
- 15. Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14(10):e275-e444.
- 16. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation. J Am Coll Cardiol. 2019;74(1):104-132.
- 17. Crijns HJ, Weijs B, Fairley AM, et al. Contemporary real life cardioversion of atrial fibrillation: Results from the multinational RHYTHM-AF study. Int J Cardiol. 2014;172(3):588-594.