📋 Key Information Summary
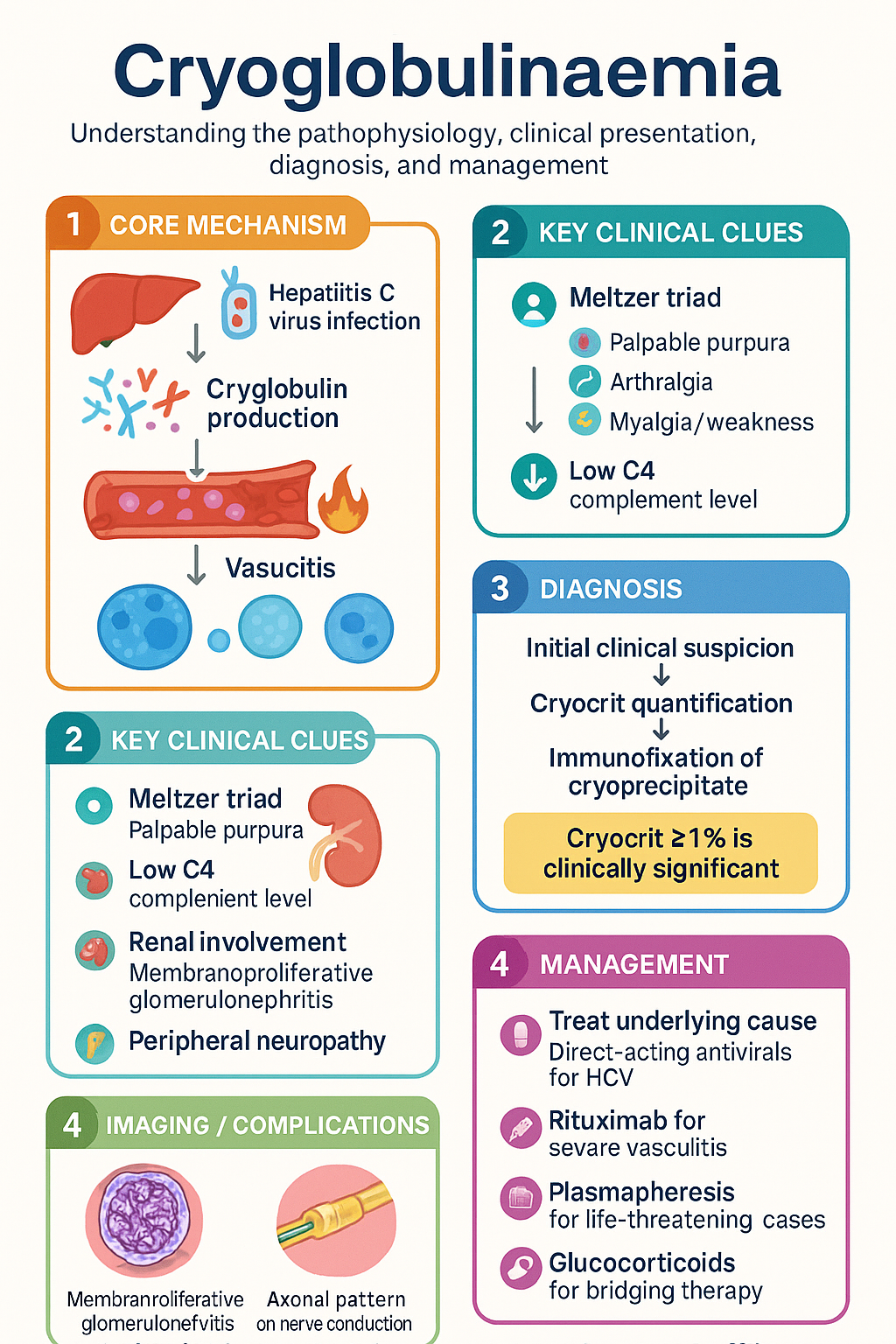
- Cryoglobulins are immunoglobulins that reversibly precipitate at temperatures <37 °C, causing small-to-medium vessel vasculitis via immune-complex deposition.
- Three types: Type I (monoclonal IgG or IgM; associated with haematological malignancy); Type II (mixed, monoclonal + polyclonal; majority HCV-associated); Type III (polyclonal; HCV, SLE, Sjögren).
- Hepatitis C virus (HCV) infection is the commonest cause of mixed cryoglobulinaemia (Types II & III), accounting for ~90% of cases in endemic regions.
- Characteristically very low C4 complement level (often the first clue); C3 may be normal or mildly reduced.
- Meltzer triad — palpable purpura, arthralgia, myalgia/weakness — is the classic clinical presentation of mixed cryoglobulinaemic vasculitis.
- Renal involvement (membranoproliferative glomerulonephritis) and peripheral neuropathy are important organ manifestations that determine prognosis.
- Diagnosis requires cryocrit >1% with characterisation by immunofixation; blood must be collected and transported at 37 °C (warm-clotted tube).
- Anti-HCV serology, HBV, HIV, ANA, RF, and serum protein electrophoresis (SPEP) with immunofixation are essential workup.
- Treatment of the underlying cause is paramount: direct-acting antiviral (DAA) therapy for HCV-associated cryoglobulinaemia (PBS-listed).
- Rituximab (MabThera®) is first-line immunosuppressive therapy for severe or refractory mixed cryoglobulinaemic vasculitis; PBS Authority Required for vasculitis indication.
- Plasmapheresis (plasma exchange) is reserved for life-threatening or rapidly progressive disease (acute GN, digital necrosis, severe neuropathy).
- Glucocorticoids (pulse IV methylprednisolone then oral prednisolone) bridge therapy while awaiting rituximab efficacy or antiviral response.
- Type I cryoglobulinaemia management targets the underlying B-cell lymphoproliferative disorder; chemotherapy ± plasmapheresis for hyperviscosity.
Introduction & Australian Epidemiology
Cryoglobulins are serum immunoglobulins that reversibly precipitate at temperatures below 37 °C and re-dissolve upon rewarming. Their presence in the circulation can lead to immune-complex deposition in small- and medium-sized vessels, producing a systemic vasculitis known as cryoglobulinaemic vasculitis.
In Australia, mixed cryoglobulinaemia (Types II and III) is predominantly associated with chronic hepatitis C virus (HCV) infection. Despite Australia's success in reducing HCV prevalence through direct-acting antiviral (DAA) programmes since 2016, cryoglobulinaemic vasculitis persists in patients with longstanding or previously treated HCV infection. The Australian Institute of Health and Welfare (AIHW) estimates approximately 180,000 people are living with chronic HCV nationally, of whom up to 40–60% may develop low-level cryoglobulins, though clinically significant vasculitis occurs in a smaller subset (~5–10%).
Type I cryoglobulinaemia is rare and is associated with haematological malignancies, particularly Waldenström macroglobulinaemia and multiple myeloma. Non-HCV causes of mixed cryoglobulinaemia in the Australian context include systemic lupus erythematosus (SLE), Sjögren syndrome, and other autoimmune conditions. Aboriginal and Torres Strait Islander peoples have a higher prevalence of HCV and autoimmune disease, requiring specific clinical consideration.
This guideline provides an Australian-focused approach to the classification, diagnosis, and management of cryoglobulinaemia, aligned with current evidence and Australian prescribing frameworks.
Types & Associations
Cryoglobulins are classified into three types based on the Brouet classification, which has important implications for aetiology, clinical features, and management strategy.
| Feature | Type I | Type II (Mixed) | Type III (Mixed) |
|---|---|---|---|
| Composition | Monoclonal IgG or IgM (rarely IgA) | Monoclonal IgM (usually IgMκ with RF activity) + polyclonal IgG | Polyclonal IgM (with RF activity) + polyclonal IgG |
| Brouet frequency | ~10–15% | ~50–60% | ~30–40% |
| Mechanism | Hyperviscosity / vascular occlusion (not immune-complex) | Immune-complex deposition; RF activity of monoclonal IgM | Immune-complex deposition; polyclonal RF |
| Key associations | Waldenström macroglobulinaemia, multiple myeloma, CLL, MGUS | HCV (~90%), HBV, HIV, Sjögren syndrome, SLE | HCV, SLE, Sjögren syndrome, other autoimmune diseases |
| Typical vasculitis | No (occlusive rather than inflammatory) | Yes — small vessel | Yes — small vessel |
| C4 | Normal or mildly low | Very low (characteristic) | Very low (characteristic) |
| RF | Negative | Positive (high titre) | Positive (variable titre) |
HCV — The Commonest Cause
Hepatitis C virus drives mixed cryoglobulinaemia through chronic antigenic stimulation of B lymphocytes, leading to clonal expansion of RF-producing B cells. In Australia, HCV genotype 1 (1a and 1b) predominates. Cryoglobulins may persist for years after HCV virological cure (SVR), and vasculitis can occasionally flare in the post-SVR period.
Other Associations
- Sjögren syndrome: Cryoglobulins present in 5–15%; their presence predicts lymphoma risk and is a criterion for severe disease in the EULAR-SSDAI.
- SLE: Mixed cryoglobulins may be detected; low C4 is common in SLE regardless.
- HBV: Less common than HCV in Australia but should be excluded.
- HIV: Polyclonal B-cell activation may produce cryoglobulins.
- Other: Rheumatoid arthritis, malignancy (non-haematological), and rare idiopathic forms.
Clinical Manifestations & Diagnosis
Meltzer Triad
The classic presentation of mixed cryoglobulinaemic vasculitis (Types II/III) is the Meltzer triad:
- Palpable purpura — typically lower limbs, triggered by cold exposure or prolonged standing; may be chronic and recurrent.
- Arthralgia — usually non-erosive, affecting knees, hands, and ankles symmetrically.
- Weakness / myalgia — constitutional symptom; may be prominent.
Organ Involvement
| System | Manifestation | Notes |
|---|---|---|
| Skin | Palpable purpura, livedo reticularis, digital ulceration, necrosis | Most common manifestation (~90%); Raynaud phenomenon |
| Renal | Membranoproliferative glomerulonephritis (MPGN) | 20–30%; proteinuria, haematuria, declining eGFR; Type I MPGN pattern on biopsy |
| Peripheral nerve | Peripheral neuropathy — sensory > motor; mononeuritis multiplex | ~60–70%; often early and disabling; axonal pattern on NCS |
| GI | Abdominal pain, mesenteric vasculitis (rare) | Ischaemic colitis in severe cases |
| Pulmonary | Interstitial lung disease, pulmonary haemorrhage (rare) | More common in Type I |
| CNS | Rare — stroke, transverse myelitis | Consider in differential of young stroke |
| Type I-specific | Hyperviscosity syndrome — visual disturbance, headache, mucosal bleeding | Acute emergency; plasmapheresis indicated |
Diagnostic Approach
The diagnosis of cryoglobulinaemic vasculitis requires both the detection of circulating cryoglobulins AND clinical evidence of vasculitis. Cryoglobulinaemia alone (without vasculitis) does not mandate immunosuppressive therapy.
Investigations
Risk Stratification & Severity Scoring
Severity assessment guides the intensity of treatment. The following classification, adapted from the Italian Group for the Study of Cryoglobulinaemia and the EULAR recommendations, stratifies mixed cryoglobulinaemic vasculitis:
Empirical Therapy
Empirical therapy is initiated before a complete aetiological workup is finalised, or while awaiting response to definitive treatment (e.g., antiviral therapy). The approach varies by severity.
Mild Disease — Symptomatic & Supportive
- Cold avoidance (warm clothing, heated environments) — fundamental but often under-emphasised.
- Compression stockings for dependent purpura.
- NSAIDs for arthralgia (avoid if renal impairment).
- Low-dose oral prednisolone (10–15 mg/day) may be used short-term for flares.
Moderate Disease — Glucocorticoids
Severe Disease — IV Pulse Methylprednisolone
Directed / Cause-Specific Therapy
HCV-Associated Mixed Cryoglobulinaemia
Antiviral therapy is the cornerstone of treatment for HCV-associated mixed cryoglobulinaemia. Direct-acting antivirals (DAAs) have transformed outcomes, with SVR rates >95% across most genotypes.
Immunosuppressive Therapy — Rituximab
Rituximab is the preferred immunosuppressive agent for moderate-to-severe mixed cryoglobulinaemic vasculitis, based on the RITUXVAS trial and multiple observational studies demonstrating superiority over conventional immunosuppression.
Plasmapheresis (Plasma Exchange)
Plasmapheresis physically removes circulating cryoglobulins and is reserved for severe, life-threatening manifestations.
- Rapidly progressive glomerulonephritis with declining renal function
- Severe digital necrosis / gangrene
- Hyperviscosity syndrome (Type I)
- Severe neuropathy with motor involvement
- Pulmonary haemorrhage
Type I Cryoglobulinaemia
Management targets the underlying B-cell lymphoproliferative disorder. Treatment is guided by haematology and follows the specific malignancy protocol (e.g., Bortezomib-Rituximab-Dexamethasone for Waldenström macroglobulinaemia, or R-CHOP for aggressive lymphoma). Plasmapheresis is indicated for hyperviscosity crisis. Rituximab monotherapy is appropriate for indolent disease.
HCV-Negative Mixed Cryoglobulinaemia
For cryoglobulinaemia associated with SLE, Sjögren syndrome, or other autoimmune conditions, rituximab combined with glucocorticoids is the preferred immunosuppressive strategy. Cyclophosphamide is reserved for refractory cases.
Monitoring
Ongoing monitoring assesses treatment response, disease activity, and complications of therapy.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Muchtar E, Magen H, Gertz MA. How I treat cryoglobulinemia. Blood. 2017;129(3):289-298. doi:10.1182/blood-2016-09-719773
- 2. Brouet JC, Clauvel JP, Danon F, Klein M, Seligmann M. Biologic and clinical significance of cryoglobulins. A report of 86 cases. Am J Med. 1974;57(5):775-788. doi:10.1016/0002-9343(74)90852-3
- 3. De Vita S, Quartuccio L, Isola M, et al. A randomized controlled trial of rituximab for the treatment of severe cryoglobulinemic vasculitis. Arthritis Rheum. 2012;64(3):843-853. doi:10.1002/art.34331
- 4. Roccatello D, Sciascia S, Baldovino S, et al. A multicentre study of the RITUXVAS trial: rituximab in cryoglobulinaemic vasculitis. RMD Open. 2018;4(2):e000662. doi:10.1136/rmdopen-2018-000662
- 5. Ferri C, Sebastiani M, Giuggioli D, et al. Mixed cryoglobulinemia: demographic, clinical, and serologic features and survival in 231 patients. Semin Arthritis Rheum. 2004;33(6):355-374. doi:10.1016/j.semarthrit.2003.10.001
- 6. Australian Institute of Health and Welfare (AIHW). Hepatitis C in Australia 2024. Canberra: AIHW; 2024. Cat. no. HIV 13.
- 7. The Royal Australian College of General Practitioners (RACGP). Hepatitis B and C: Testing, Management and Treatment. 4th edition. East Melbourne: RACGP; 2022.
- 8. Mukhtyar C, Guillevin L, Cid MC, et al. EULAR recommendations for the management of primary small and medium vessel vasculitis. Ann Rheum Dis. 2009;68(3):310-317. doi:10.1136/ard.2008.088096
- 9. Cacoub P, Comarmond C, Domont F, Savey L, Desbois AC, Saadoun D. Extrahepatic manifestations of chronic hepatitis C virus infection. Ther Adv Infect Dis. 2016;3(1):3-14. doi:10.1177/2049936115585942
- 10. Dammacco F, Sansonno D. Therapy for hepatitis C virus-related cryoglobulinemic vasculitis. N Engl J Med. 2013;369(11):1035-1045. doi:10.1056/NEJMra1208642
- 11. RHDAustralia (Northern Territory Department of Health and Menzies School of Health Research). Australian Guidelines for the Prevention, Diagnosis and Management of Acute Rheumatic Fever and Rheumatic Heart Disease. 3rd edition. Darwin: RHDAustralia; 2020.
- 12. Australasian Society for Clinical Immunology and Allergy (ASCIA). Position statement on the use of rituximab in autoimmune conditions. Sydney: ASCIA; 2023.
- 13. Pharmaceutical Benefits Scheme (PBS). Schedule of Pharmaceutical Benefits. Australian Government Department of Health and Aged Care. Available at: www.pbs.gov.au. Accessed 2024.
- 14. National Aboriginal Community Controlled Health Organisation (NACCHO). Position statement on hepatitis C elimination in Aboriginal and Torres Strait Islander communities. Canberra: NACCHO; 2023.