📋 Key Information Summary
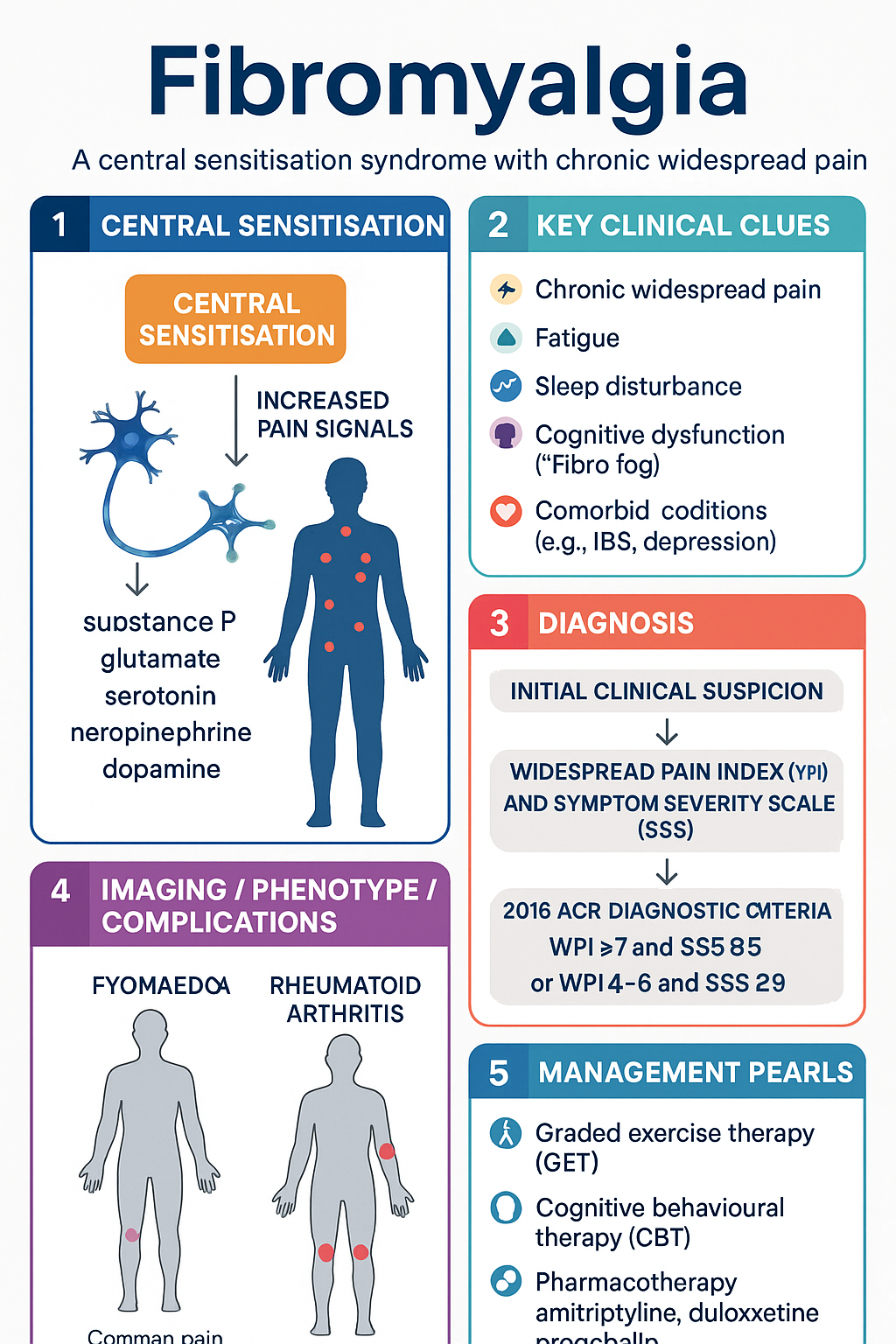
- Fibromyalgia is a central sensitisation syndrome characterised by chronic widespread pain (CWP), fatigue, sleep disturbance, and cognitive dysfunction — diagnosis is clinical, supported by the 2016 ACR Preliminary Diagnostic Criteria.
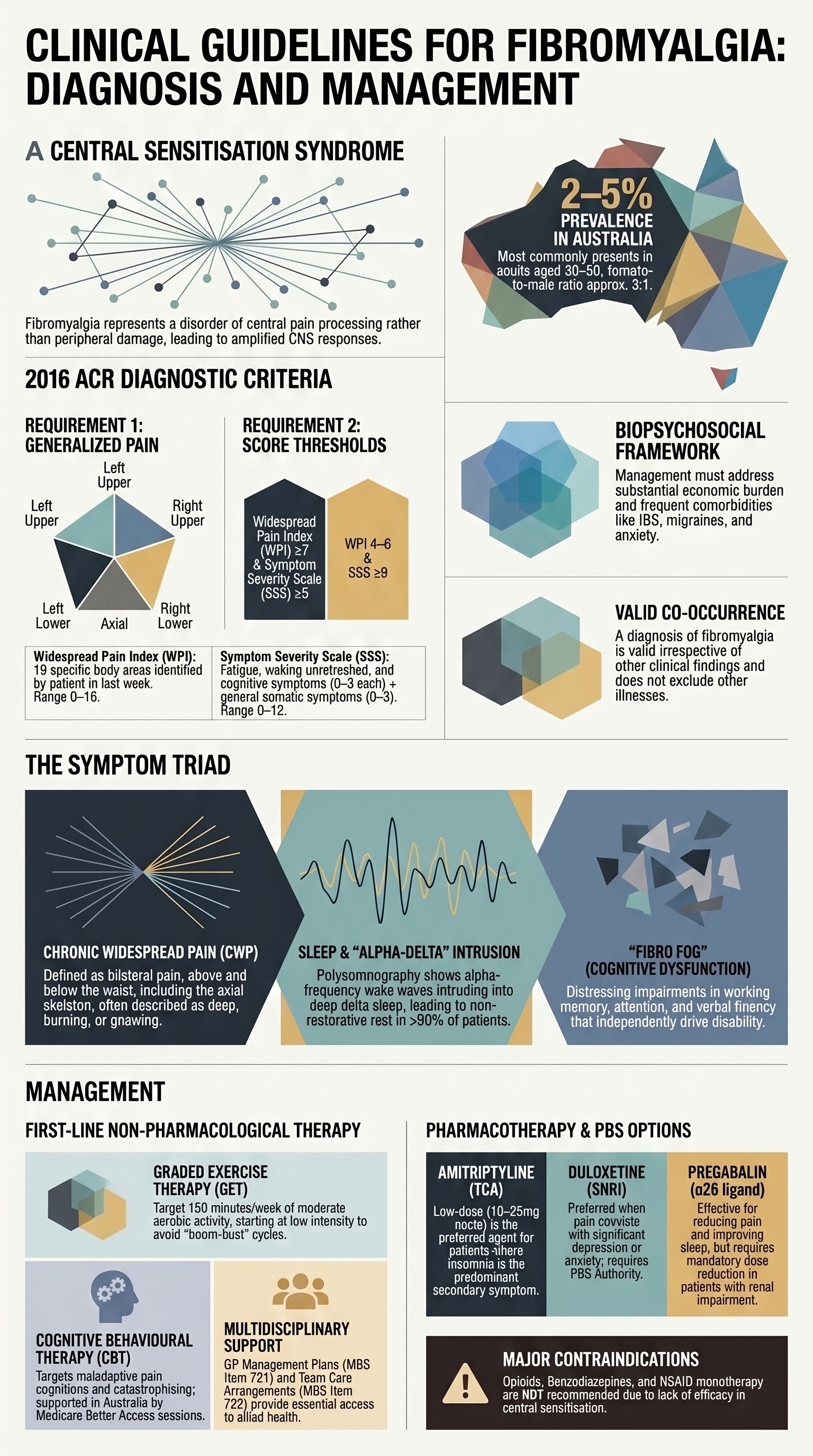
- The 2016 ACR criteria use the Widespread Pain Index (WPI) and Symptom Severity Scale (SSS); generalised pain in ≥4 of 5 body regions plus SSS ≥9 (or WPI 4–6 + SSS ≥12) meets the threshold, with symptoms present ≥3 months.
- Chronic widespread pain is the hallmark feature — must be present for ≥3 months, typically bilateral, above and below the waist, and involving the axial skeleton.
- Fatigue and non-restorative sleep are near-universal; poor sleep quality amplifies pain perception and functional impairment.
- "Fibro fog" (cognitive dysfunction) affects concentration, working memory, and multitasking; it is an independent driver of disability and reduced quality of life.
- Non-pharmacological therapy is first-line: graded exercise therapy (GET) and cognitive behavioural therapy (CBT) have the strongest evidence base and should be initiated before or alongside pharmacotherapy.
- Three medications are PBS-listed for fibromyalgia in Australia — amitriptyline (low-dose), duloxetine (SNRI), and pregabalin (α2δ ligand) — all considered first-line pharmacological options.
- Amitriptyline 10–25 mg nocte is a well-established, inexpensive first-line option; titrate cautiously to 50 mg if tolerated; anticholinergic side effects limit dose escalation.
- Duloxetine 60 mg daily (range 30–120 mg) is effective for pain, fatigue, and comorbid depression/anxiety; PBS Authority Required for fibromyalgia.
- Pregabalin 150–450 mg/day in divided doses reduces pain and improves sleep; dose-reduce in renal impairment (eGFR <60); PBS Authority Required for fibromyalgia.
- Opioids, benzodiazepines, and NSAIDs as monotherapy are NOT recommended — they lack efficacy in central sensitisation pain and carry significant harm.
- ATSI Australians have higher prevalence of chronic pain and CWP; culturally safe, multidisciplinary care and remote-access strategies are essential.
- Comorbid anxiety, depression, and irritable bowel syndrome are common; a biopsychosocial approach addressing all domains improves outcomes.
- Diagnosis should exclude inflammatory rheumatological disease, hypothyroidism, and other causes of widespread pain — but avoid excessive investigation once red flags are excluded.
- Shared decision-making, patient education about central sensitisation, and realistic goal-setting are foundational to successful management.
Introduction & Australian Epidemiology
Fibromyalgia is a chronic, centralised pain syndrome characterised by widespread musculoskeletal pain accompanied by fatigue, sleep disturbance, memory difficulties, and mood disturbance. It is classified among the central sensitisation syndromes and represents a disorder of pain processing rather than peripheral tissue damage.
In Australia, the prevalence of fibromyalgia is estimated at 2–5% of the adult population, with a female-to-male ratio of approximately 3:1. The condition is seen across all age groups but most commonly presents between ages 30 and 60 years. The Australian Institute of Health and Welfare (AIHW) identifies chronic widespread pain as a significant contributor to disability and healthcare utilisation.
Fibromyalgia frequently coexists with other conditions including irritable bowel syndrome (IBS), temporomandibular joint disorder, tension-type headache, migraine, interstitial cystitis, chronic fatigue syndrome, depression, and anxiety. The biopsychosocial model is the accepted framework for understanding and managing fibromyalgia in Australian practice.
The economic burden is substantial, with significant costs relating to healthcare visits, medications, lost productivity, and disability payments. Early recognition and evidence-based management can reduce this burden and improve patient outcomes.
2016 ACR Diagnostic Criteria
The 2016 Revisions to the 2010 American College of Rheumatology (ACR) Preliminary Diagnostic Criteria for Fibromyalgia are the current standard for clinical diagnosis. These criteria replaced the 1990 tender-point examination and can be applied in both clinical and research settings.
- Generalised pain defined as pain in ≥4 of 5 body regions (left upper, right upper, left lower, right lower, axial) — jaw, chest, and abdominal pain may be included.
- Symptoms present at a similar level for ≥3 months.
- Widespread Pain Index (WPI) ≥7 and Symptom Severity Scale (SSS) ≥5, OR WPI 4–6 and SSS ≥9.
- A diagnosis of fibromyalgia is valid irrespective of other diagnoses; it does not exclude the presence of other clinically important illnesses.
Widespread Pain Index (WPI)
The patient identifies areas of pain in the prior week from a list of 19 body areas. Score 0–19.
| Body Region | Areas Scored |
|---|---|
| Left upper | Shoulder girdle, upper arm, lower arm |
| Right upper | Shoulder girdle, upper arm, lower arm |
| Left lower | Hip, upper leg, lower leg |
| Right lower | Hip, upper leg, lower leg |
| Axial | Jaw (L & R), upper back, lower back, chest, abdomen, neck |
Symptom Severity Scale (SSS)
Rate each of three symptoms (fatigue, waking unrefreshed, cognitive symptoms) on a 0–3 scale (0 = no problem, 3 = severe, pervasive, continuous, life-disturbing). Add the score of somatic symptoms in general (0–3). Total score range: 0–12.
2016 Revisions — Key Changes
- The requirement for a separate clinical diagnosis of fibromyalgia by a physician was removed — self-report and physician-applied criteria are equivalent.
- The term "generalised pain" replaced the earlier descriptor to allow inclusion of jaw, chest, and abdominal pain.
- The criteria acknowledge that fibromyalgia can coexist with other rheumatic and non-rheumatic conditions — it is not a diagnosis of exclusion.
- The polysymptomatic distress scale (PSD = WPI + SSS, range 0–31) can track disease severity longitudinally.
Differential Diagnoses to Exclude
Before confirming fibromyalgia, the following should be considered and excluded where clinically appropriate:
- Inflammatory rheumatic diseases — rheumatoid arthritis, systemic lupus erythematosus, polymyalgia rheumatica, spondyloarthropathy
- Endocrine disorders — hypothyroidism, hyperparathyroidism, acromegaly, Cushing syndrome
- Neurological conditions — multiple sclerosis, myasthenia gravis, small fibre neuropathy
- Infections — hepatitis C, HIV, Lyme disease (rare in Australia)
- Medications — statins, aromatase inhibitors, proton pump inhibitors
- Vitamin D deficiency, iron deficiency, and obstructive sleep apnoea should be assessed
Chronic Widespread Pain
Chronic widespread pain (CWP) is the cardinal symptom of fibromyalgia and the primary reason patients seek medical attention. It is defined as pain present for ≥3 months, affecting both sides of the body, above and below the waist, and involving the axial skeleton (cervical spine, anterior chest, thoracic spine, or low back).
Pathophysiology of Central Sensitisation
CWP in fibromyalgia results from amplified central nervous system pain processing — termed central sensitisation. Key mechanisms include:
- Ascending facilitation: Increased excitability of dorsal horn neurons leads to wind-up and expanded receptive fields.
- Descending inhibition failure: Reduced serotonergic and noradrenergic descending inhibitory pathways fail to modulate nociceptive input.
- Neurochemical imbalance: Elevated substance P and glutamate in cerebrospinal fluid; reduced serotonin, norepinephrine, and dopamine.
- Functional brain changes: fMRI studies demonstrate augmented pain-processing regions (insula, anterior cingulate cortex, somatosensory cortex) at equivalent stimulus intensity.
- Small fibre neuropathy: Skin biopsy studies in a subset of patients show reduced intraepidermal nerve fibre density, suggesting peripheral contribution in some cases.
Clinical Features of CWP in Fibromyalgia
- Pain is typically described as deep, aching, burning, or gnawing; may fluctuate in intensity
- Exacerbated by stress, cold, poor sleep, physical inactivity, and hormonal changes
- Allodynia (pain from normally non-painful stimuli) and hyperalgesia (amplified pain response) are common
- Pain may migrate between regions; whole-body pain flares are characteristic
- Comorbid regional pain syndromes (e.g., myofascial pain, tension headache) frequently overlap
Fatigue & Sleep Disturbance
Fatigue and sleep disturbance are core symptoms of fibromyalgia, present in >90% of patients. They are bidirectionally related to pain — poor sleep amplifies pain perception, and pain disrupts sleep architecture.
Fatigue
Fatigue in fibromyalgia is typically described as overwhelming, persistent, and disproportionate to exertion. It differs from normal tiredness in its persistence despite rest and its interference with daily function.
- Present on waking and worsens throughout the day in many patients
- May be exacerbated by physical activity, cognitive tasks, and emotional stress
- Significantly impacts work capacity, social engagement, and quality of life
- Contributes to deconditioning and social withdrawal if not addressed
Sleep Disturbance
Polysomnographic studies reveal characteristic sleep abnormalities in fibromyalgia:
- Alpha-delta sleep: Intrusion of alpha-frequency (wake) waves into delta (deep) sleep — the most consistent polysomnographic finding
- Reduced slow-wave (Stage N3) sleep and fragmented sleep architecture
- Increased periodic limb movements of sleep (PLMS) and restless legs syndrome
- Non-restorative sleep — patients wake feeling unrefreshed regardless of sleep duration
- Comorbid obstructive sleep apnoea should be assessed, especially in patients with BMI ≥30 or significant snoring
Management of Fatigue and Sleep
- Sleep hygiene education — consistent bedtime, dark/cool room, limit screens, avoid caffeine after midday
- CBT for insomnia (CBT-I) — evidence-based, improves sleep quality and fatigue
- Low-dose amitriptyline (10–25 mg nocte) improves sleep quality and reduces pain; anticholinergic effects may limit use
- Pregabalin improves sleep architecture and reduces pain — useful when sleep disruption is prominent
- Graded exercise therapy improves fatigue and sleep over time — even modest increases in activity are beneficial
- Melatonin (2–3 mg nocte) may be trialled for circadian disturbance; limited evidence in fibromyalgia specifically
Cognitive Symptoms ("Fibro Fog")
Cognitive dysfunction, colloquially termed "fibro fog," is a well-recognised and often distressing feature of fibromyalgia. It is included in the 2016 ACR criteria as one of three SSS symptom domains.
Cognitive Domains Affected
- Working memory: Difficulty holding information in mind (e.g., phone numbers, instructions)
- Attention and concentration: Easily distracted, difficulty sustaining focus on tasks
- Executive function: Impaired planning, multitasking, and decision-making
- Verbal fluency: Word-finding difficulties, tip-of-the-tongue phenomena
- Processing speed: Slower information processing, particularly under time pressure
Contributing Factors
Fibro fog is multifactorial and exacerbated by:
- Sleep deprivation and non-restorative sleep
- Chronic pain — attentional resources diverted to pain processing
- Comorbid depression and anxiety
- Medication side effects (opioids, benzodiazepines, first-generation antihistamines)
- Physical deconditioning and reduced aerobic fitness
Management
- Address underlying contributors — optimise sleep, treat depression/anxiety, review medications
- CBT improves cognitive function indirectly through pain and mood improvement
- Graded exercise improves cerebral perfusion and cognitive outcomes
- Cognitive pacing — breaking tasks into manageable segments with rest breaks
- Neuropsychological rehabilitation may benefit selected patients with significant impairment
- Avoid opioids and benzodiazepines which worsen cognitive function
Non-Pharmacological Therapy
Non-pharmacological therapy is the cornerstone of fibromyalgia management and should be first-line, initiated before or concurrently with pharmacotherapy. The strongest evidence supports graded exercise therapy and cognitive behavioural therapy.
Graded Exercise Therapy (GET)
Regular aerobic exercise is one of the most effective interventions for fibromyalgia, with benefits across pain, fatigue, sleep, and mood domains.
- Start at low intensity (e.g., walking 10–15 minutes, 3 times/week) and gradually increase over weeks to months
- Target: 150 minutes/week of moderate-intensity aerobic activity (e.g., brisk walking, swimming, cycling)
- Aquatic exercise is particularly well-tolerated — warm water reduces pain and supports movement
- Resistance training 2–3 times/week improves strength, function, and pain
- Tai chi and yoga have moderate evidence for fibromyalgia — improve pain, sleep, and quality of life
- Exercise should be self-paced and gradually progressed; avoid boom-bust cycles
Cognitive Behavioural Therapy (CBT)
CBT is the psychological therapy with the strongest evidence base for fibromyalgia. It targets maladaptive pain cognitions, catastrophising, and avoidance behaviours.
- Typically 6–12 sessions delivered by a psychologist experienced in chronic pain
- Reduces pain intensity, improves function, and decreases healthcare utilisation
- Addresses catastrophising, fear-avoidance, and pain self-efficacy
- Acceptance and Commitment Therapy (ACT) is an emerging alternative with growing evidence
- Telehealth delivery is effective and improves access for rural/remote patients
- Medicare Better Access initiative provides up to 10 individual and 10 group sessions per year with a GP Mental Health Treatment Plan
Other Non-Pharmacological Approaches
| Intervention | Evidence Level | Key Considerations |
|---|---|---|
| Patient education | Strong | Explanation of central sensitisation model; reduces catastrophising |
| Sleep hygiene / CBT-I | Strong | Improves sleep quality; reduces pain amplification |
| Multidisciplinary pain programme | Strong | Combines physiotherapy, psychology, occupational therapy |
| Acupuncture | Moderate | Short-term pain relief; may be trialled as adjunct |
| Mindfulness-based stress reduction | Moderate | Reduces pain catastrophising and improves coping |
| Hydrotherapy / balneotherapy | Moderate | Warm water exercise well-tolerated; improves pain and function |
Australian Medicare Support
- GP Management Plan (GPMP) — MBS Item 721: Enables up to 5 individual allied health services per calendar year
- Team Care Arrangement (TCA) — MBS Item 723: Coordinates multidisciplinary care
- Mental Health Treatment Plan — MBS Items 2700/2701: Up to 10 individual + 10 group psychology sessions per year
- Chronic Disease Management: Reviews (MBS Item 732) at least every 12 months
Pharmacotherapy
Pharmacotherapy for fibromyalgia targets the central mechanisms of pain processing. In Australia, three medications have specific PBS listings for fibromyalgia: amitriptyline, duloxetine, and pregabalin. All are considered first-line, and the choice depends on the patient's symptom profile, comorbidities, and tolerability.
First-Line Pharmacotherapy
Choosing First-Line Therapy
| Clinical Scenario | Preferred Agent | Rationale |
|---|---|---|
| Pain + insomnia predominant | Amitriptyline | Improves sleep architecture; low cost (PBS General Benefit) |
| Pain + depression/anxiety | Duloxetine | Dual action on pain and mood; also licensed for GDD/MDD |
| Pain + prominent neuropathic features | Pregabalin | Effective for allodynia and hyperalgesia; improves sleep |
| Anticholinergic intolerance (elderly) | Duloxetine or Pregabalin | Avoid TCA side effects in older patients |
| Obesity / weight concerns | Duloxetine | Weight-neutral; amitriptyline and pregabalin associated with weight gain |
Combination Therapy
If monotherapy provides inadequate response, combination of agents from different classes may be considered (e.g., amitriptyline + pregabalin, or duloxetine + pregabalin). Evidence is limited but supported by clinical practice. Avoid combining duloxetine and amitriptyline (serotonin syndrome risk — generally low but monitor).
Agents NOT Recommended / Limited Evidence
| Agent | Recommendation | Rationale |
|---|---|---|
| Opioids (tramadol, oxycodone, codeine) | NOT recommended | No efficacy in central sensitisation; risk of dependence, hyperalgesia |
| NSAIDs | NOT as monotherapy | Lack central mechanism; may be adjunct for peripheral pain component |
| Benzodiazepines | NOT recommended | Worsen fatigue and cognition; dependence risk; no evidence |
| Gabapentin | Second-line / off-label | Less evidence than pregabalin; TID dosing; not PBS-listed for FM |
| Milnacipran | Not available in Australia | SNRI approved for FM overseas but not TGA-registered |
Monitoring
Fibromyalgia is a chronic condition requiring longitudinal management with regular review and reassessment. A structured approach to monitoring improves outcomes and reduces polypharmacy.
Monitoring Framework
- Confirm diagnosis using 2016 ACR criteria; document WPI and SSS
- Baseline bloods: FBC, EUC, LFT, TFT, HbA1c, ferritin, vitamin D, CRP/ESR
- Assess comorbid depression/anxiety (PHQ-9, GAD-7); screen for sleep apnoea if indicated
- Functional assessment and patient-defined goals
- ECG if commencing amitriptyline >25 mg or cardiac history
- Assess tolerability and side effects of pharmacotherapy
- Titrate dose if tolerated and subtherapeutic
- Review exercise adherence and CBT engagement
- Formal efficacy assessment — pain (VAS/NRS), function, sleep, mood
- If inadequate response: optimise dose, switch agent, or consider combination
- Reassess PSD score (WPI + SSS) as longitudinal measure
- Review ongoing need for medications; attempt dose reduction if stable
- Reassess functional goals; adjust management plan
- Screen for new comorbidities; review polypharmacy
- GP Management Plan review (MBS Item 732)
Special Populations
ATSI Health Considerations
📚 References
- 1. Wolfe F, Clauw DJ, Fitzcharles MA, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Seminars in Arthritis and Rheumatism. 2016;46(3):319-329.
- 2. Clauw DJ. Fibromyalgia: a clinical review. JAMA. 2014;311(15):1547-1555.
- 3. Häuser W, Ablin J, Fitzcharles MA, et al. Fibromyalgia. Nature Reviews Disease Primers. 2015;1:15022.
- 4. Macfarlane GJ, Kronisch C, Dean LE, et al. EULAR revised recommendations for the management of fibromyalgia. Annals of the Rheumatic Diseases. 2017;76(2):318-328.
- 5. Fitzcharles MA, Ste-Marie PA, Goldenberg DL, et al. 2012 Canadian guidelines for the diagnosis and management of fibromyalgia syndrome. Pain Research & Management. 2013;18(3):119-126.
- 6. Australian Institute of Health and Welfare (AIHW). Chronic pain in Australia. Cat. no. PHE 267. Canberra: AIHW; 2020.
- 7. The Royal Australian College of General Practitioners (RACGP). General practice management of type 2 diabetes and chronic pain: a handbook for clinical practice. East Melbourne: RACGP; 2020.
- 8. Bidonde J, Busch AJ, Webber SC, et al. Aquatic exercise training for fibromyalgia. Cochrane Database of Systematic Reviews. 2014;(10):CD011336.
- 9. Bernardy K, Klose P, Busch AJ, et al. Cognitive behavioural therapies for fibromyalgia. Cochrane Database of Systematic Reviews. 2013;(9):CD009796.
- 10. Derry S, Cording M, Wiffen PJ, et al. Pregabalin for pain in fibromyalgia in adults. Cochrane Database of Systematic Reviews. 2016;9:CD011790.
- 11. Lunn MP, Hughes RA, Wiffen PJ. Duloxetine for treating painful neuropathy, chronic pain or fibromyalgia. Cochrane Database of Systematic Reviews. 2014;(1):CD007115.
- 12. Häuser W, Walitt B, Fitzcharles MA, et al. Review of pharmacological therapies in fibromyalgia syndromes. Arthritis Research & Therapy. 2014;16(1):201.
- 13. National Health and Medical Research Council (NHMRC). Australian guidelines to reduce health risks from drinking alcohol. Canberra: NHMRC; 2020.
- 14. Pharmaceutical Benefits Scheme (PBS). Australian Government Department of Health. Available at: https://www.pbs.gov.au. Accessed 2024.
- 15. Australian Government Department of Health. Medicare Benefits Schedule (MBS) — Chronic Disease Management items. Available at: http://www.mbsonline.gov.au. Accessed 2024.