📋 Key Information Summary
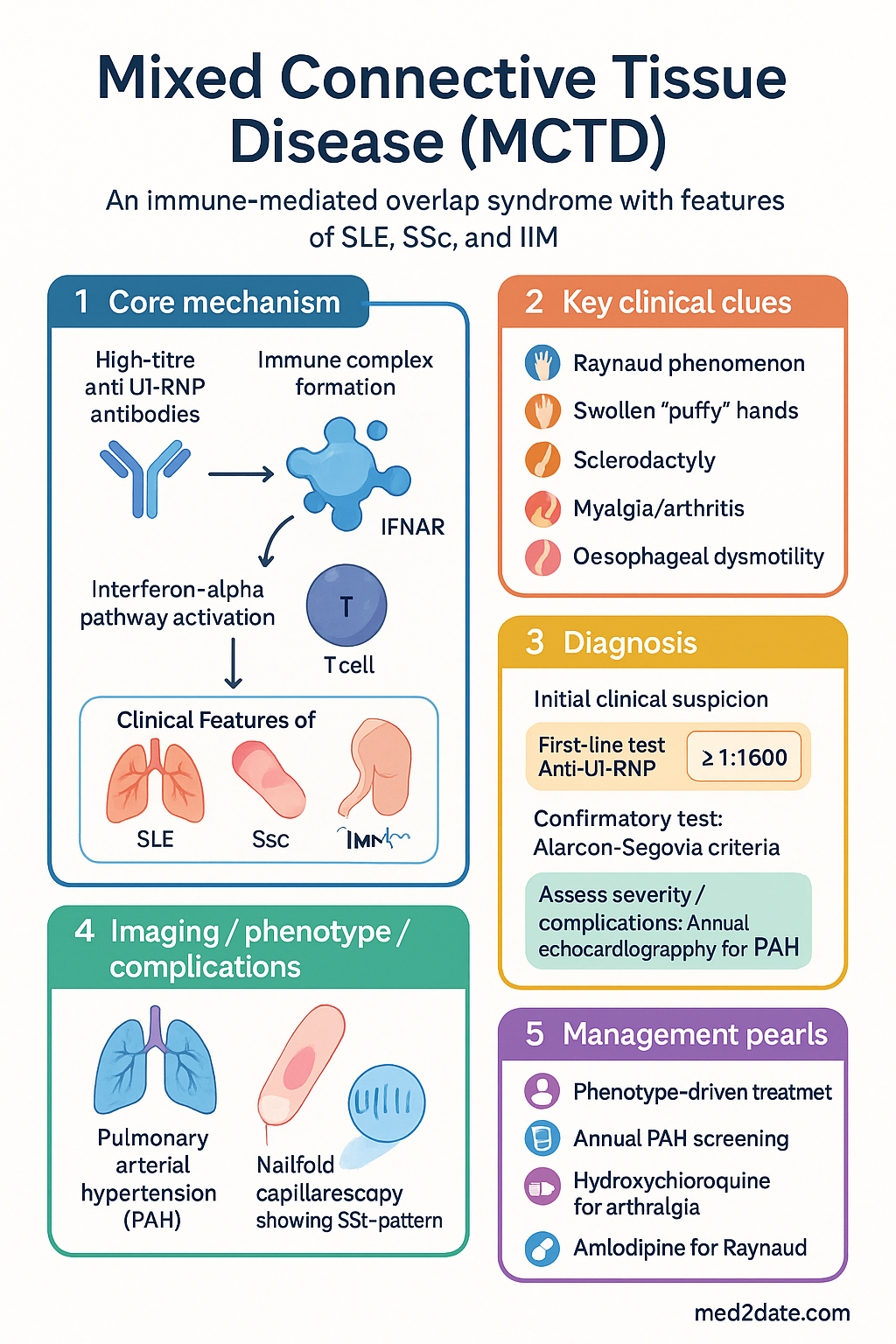
- Definition: Mixed Connective Tissue Disease (MCTD) is an immune-mediated overlap syndrome defined by high-titre anti-U1-RNP antibodies and clinical features of SLE, systemic sclerosis (SSc), and polymyositis/dermatomyositis (IIM).
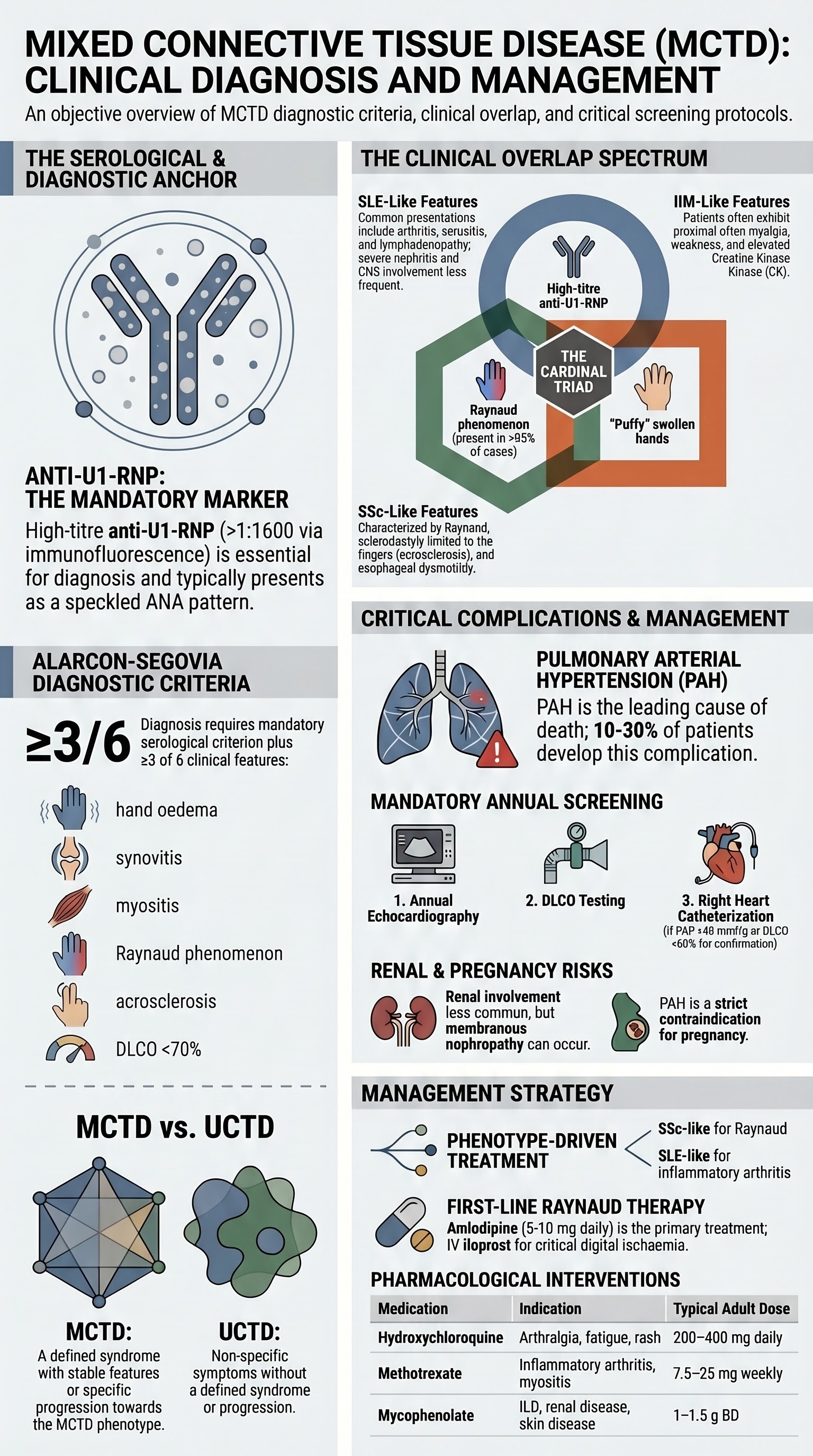
- Core antibody: High-titre anti-U1-RNP (nucleolar pattern on ANA) is mandatory for diagnosis and often precedes clinical features.
- Cardinal features: Raynaud phenomenon (nearly universal), swollen "puffy" hands (sausage digits), sclerodactyly, myalgia/arthritis, and oesophageal dysmotility.
- Most feared complication: Pulmonary arterial hypertension (PAH) is the leading cause of death; annual screening is mandatory.
- Key differential: Differentiate from undifferentiated CTD (UCTD) by the presence of anti-U1-RNP and specific multi-system overlap features.
- Management: Base treatment on dominant phenotype (e.g., SSc-like for Raynaud/PAH, SLE-like for arthritis, IIM-like for myositis).
- PAH screening: Annual echocardiography and DLCO; right heart catheterisation for confirmation.
- Renal involvement: Less common than in SLE; membranous nephropathy is typical if it occurs.
- Prognosis: Generally favourable 10-year survival (>80%), but PAH and pulmonary fibrosis worsen outcome.
Introduction & Australian Epidemiology
Mixed Connective Tissue Disease (MCTD) is a distinct overlap syndrome characterised by high-titre antibodies to U1-ribonucleoprotein (U1-RNP) and clinical features of systemic lupus erythematosus (SLE), systemic sclerosis (SSc), polymyositis/dermatomyositis (IIM), and rheumatoid arthritis (RA).
It accounts for approximately 2-3% of systemic autoimmune rheumatic diseases in Australia. Prevalence is estimated at 1-2 per 100,000, with a strong female predominance (F:M ~9:1). Onset is typically in the second to third decade. Australian data mirror international trends, with Aboriginal and Torres Strait Islander populations potentially experiencing higher rates of severe organ involvement.
Anti-U1-RNP Antibodies
Anti-U1-RNP antibodies target the U1 small nuclear ribonucleoprotein complex. They are essential for diagnosis and are present in high titres (>1:1600 by immunofluorescence).
- Pattern: Typically a speckled ANA pattern. Anti-U1-RNP is often the sole extractable nuclear antigen (ENA).
- Pathogenic role: Contributes to immune complex formation and interferon-alpha pathway activation.
- Prognostic association: High titres correlate with Raynaud phenomenon, oesophageal dysmotility, and pulmonary hypertension.
- Testing in Australia: Available via major pathology laboratories (e.g., Sonic, Laverty). MBS rebate applies for ENA testing (item 69494).
Overlap Features (SLE, SSc, IIM)
MCTD is a true overlap, with patients displaying features from at least two of the following diseases:
| Disease Overlap | Typical Features in MCTD | Less Common in MCTD |
|---|---|---|
| SLE-like | Arthritis, serositis, lymphadenopathy, fever, leukopenia | Severe nephritis, CNS lupus, anti-dsDNA antibodies |
| SSc-like | Raynaud, sclerodactyly, swollen hands, oesophageal dysmotility, PAH | Diffuse cutaneous sclerosis (usually limited) |
| IIM-like | Proximal myalgia/weakness, elevated CK, myositis on EMG/MRI | Severe interstitial lung disease (ILD) compared to pure IIM |
Features often evolve over time. The "Sharp syndrome" original description emphasised the triad of high-titre anti-U1-RNP, swollen hands, and Raynaud.
Raynaud Phenomenon & Swollen Hands
Present in >95% of patients. Often the earliest symptom, preceding other features by years.
- Raynaud: Severe, triphasic (white-blue-red). May lead to digital pitting, ulceration, or gangrene. Assess with nailfold capillaroscopy (abnormal in ~60%, showing SSc-like pattern).
- Swollen hands: "Puffy" or sausage-digit appearance due to non-pitting oedema. A key distinguishing feature from pure SSc or SLE.
- Sclerodactyly: Often develops later, confined to fingers (acral sclerosis).
Pulmonary Hypertension
The leading cause of mortality in MCTD. Prevalence: 10-30% over disease course. Mechanism: predominantly pulmonary arterial hypertension (PAH, WHO Group 1) from vasculopathy.
- Symptoms: Exertional dyspnoea (often disproportionate to lung disease), syncope, chest pain.
- Australian centres: RHC and PAH therapy initiation restricted to specialist centres (e.g., Royal Adelaide, Alfred, St Vincent's Sydney).
- Treatment: Endothelin receptor antagonists (e.g., ambrisentan, PBS Authority Required), PDE5 inhibitors (sildenafil, PBS Authority), prostanoids (epoprostenol IV).
Diagnosis: Alarcon-Segovia Criteria
The most widely used criteria. Require both serological and clinical components.
- 1. Oedema of hands
- 2. Synovitis
- 3. Myositis (biopsy or elevated CK)
- 4. Raynaud phenomenon
- 5. Acrosclerosis (sclerodactyly)
- 6. DLCO <70% of predicted
Diagnostic validation: The clinical features must derive from at least two of the diseases: SLE, SSc, IIM, RA.
Differentiating from Undifferentiated CTD
Undifferentiated connective tissue disease (UCTD) is a provisional diagnosis for patients with suggestive symptoms and serology who do not meet criteria for a defined CTD. MCTD is a specific, defined overlap.
| Feature | MCTD | UCTD |
|---|---|---|
| Antibody | High-titre anti-U1-RNP (mandatory) | ANA often positive; anti-U1-RNP may be low-titre or absent |
| Overlap features | Clear features from ≥2 specific CTDs (SLE, SSc, IIM) | Non-specific (arthralgia, Raynaud, sicca) without definite pattern |
| Criteria | Meets Alarcon-Segovia or Sharp criteria | Does not meet criteria for any specific CTD |
| Evolution | Features stable or progress within MCTD phenotype | May evolve into a defined CTD (e.g., SLE) in 30% over 5 years |
In practice, a patient with Raynaud, arthralgia, and a positive ANA but without anti-U1-RNP or specific organ involvement is classified as UCTD.
Investigations
Management Overview
Treatment is phenotype-driven, targeting the dominant clinical syndrome.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Limited specific data on MCTD prevalence in ATSI populations. However, systemic autoimmune diseases are significant contributors to morbidity.
📚 References
- 1. Alarcón-Segovia D, Cardiel MH. Comparison between 3 diagnostic criteria for mixed connective tissue disease. Study of 593 patients. J Rheumatol. 1989;16(3):328-334.
- 2. Sharp GC, Irvin WS, Tan EM, et al. Mixed connective tissue disease—an apparently distinct rheumatic disease syndrome associated with a specific antibody to an extractable nuclear antigen (ENA). Am J Med. 1972;52(2):148-159.
- 3. Cappelli S, Bellando Randone S, Martinović D, et al. "To be or not to be," ten years after: evidence for mixed connective tissue disease as a distinct entity. Semin Arthritis Rheum. 2012;41(4):589-598.
- 4. Reiseter S, Gunnarsson R, Corander J, et al. Disease evolution in mixed connective tissue disease: results from a long-term nationwide prospective cohort study. Arthritis Res Ther. 2017;19(1):284.
- 5. Gendi NST, Welsh KI, Van Venrooij WJ, et al. HLA type as a predictor of mixed connective tissue disease differentiation: ten-year clinical and immunogenetic followup. Arthritis Rheum. 1995;38(2):259-266.
- 6. Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2017.
- 7. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework. Canberra: AIHW; 2023.
- 8. Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2016;37(1):67-119.
- 9. Tyndall AJ, Bannert B, Vonk M, et al. Causes and predictors of death in systemic sclerosis: a study from the EULAR Scleroderma Trials and Research (EUSTAR) database. Ann Rheum Dis. 2010;69(10):1809-1815.
- 10. Lundberg IE, Tjärnlund A, Bottai M, et al. 2017 European League Against Rheumatism/American College of Rheumatology classification criteria for adult and juvenile idiopathic inflammatory myopathies and their major subgroups. Arthritis Rheumatol. 2017;69(12):2271-2282.
- 11. Rhodes B, Fürnrohr BG, Vyse TJ. C-reactive protein in rheumatology: biology and genetics. Nat Rev Rheumatol. 2011;7(5):282-289.
- 12. Hughes M, Herrick AL. Digital ulcers in systemic sclerosis. Rheumatology (Oxford). 2017;56(1):14-25.