📋 Key Information Summary
- Polymyalgia rheumatica (PMR) is the most common inflammatory rheumatic disease in older Australians, with an incidence of ~80 per 100,000 person-years in those aged ≥50 years.
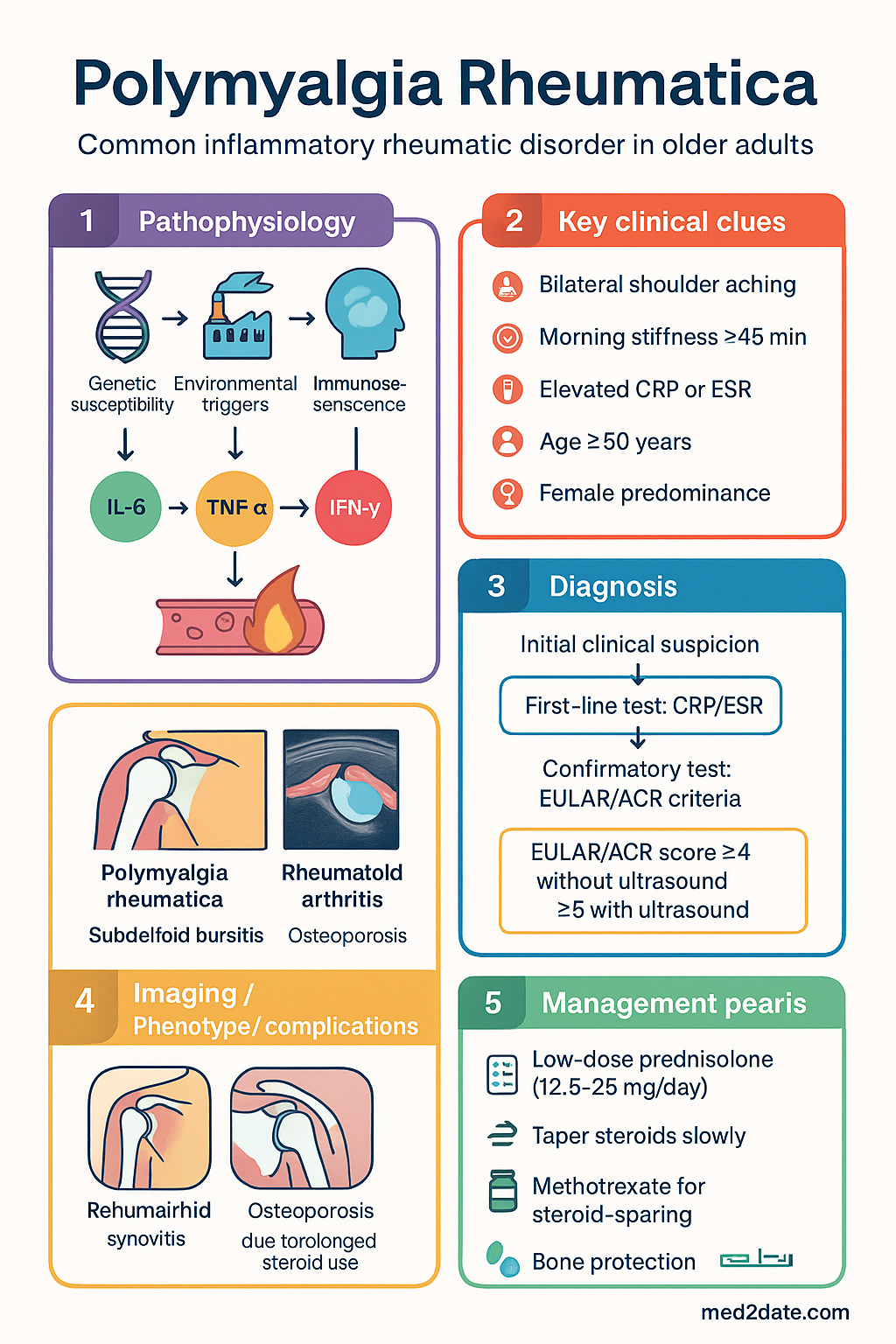
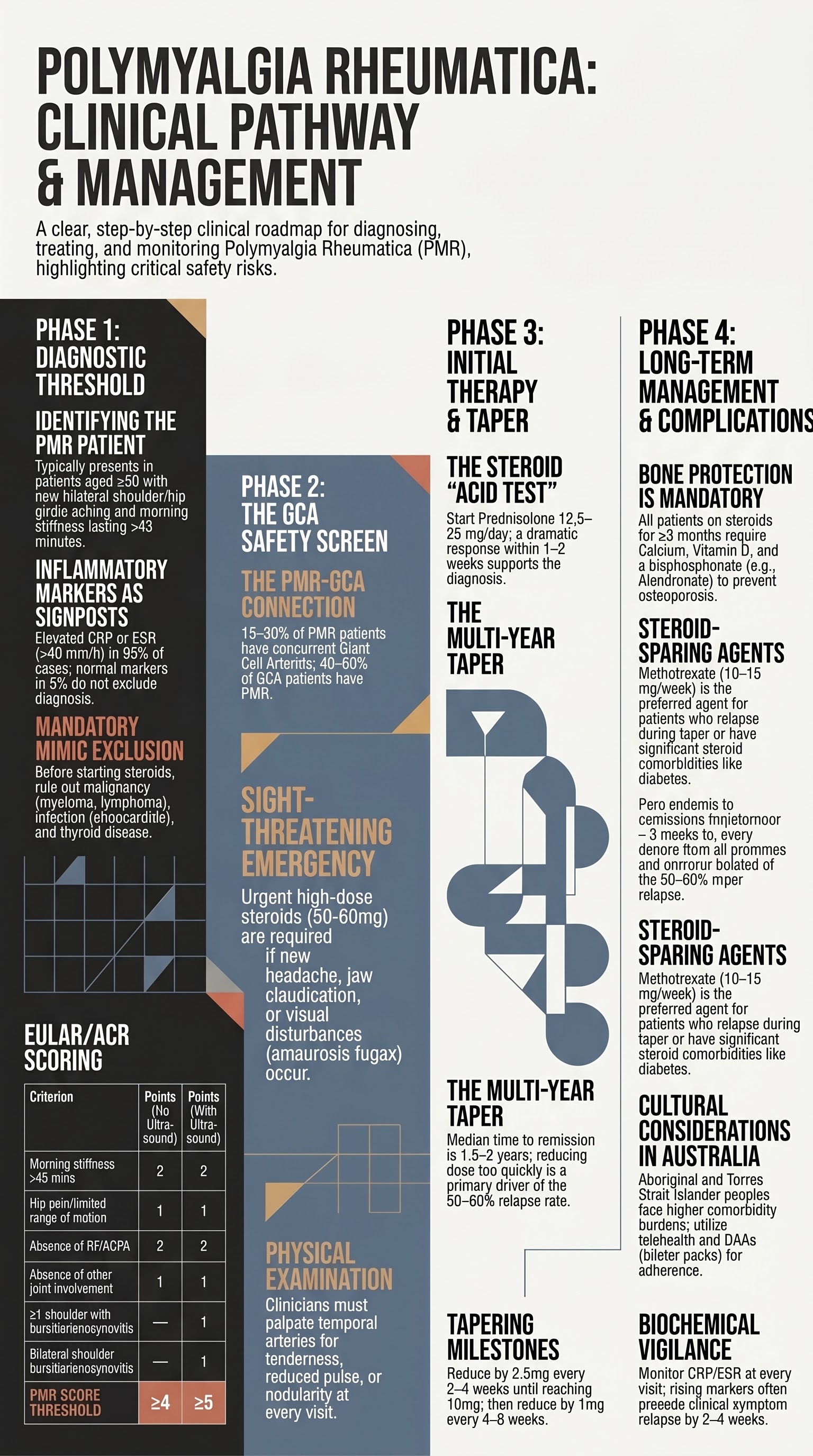
- The 2012 EULAR/ACR classification criteria (age ≥50, bilateral shoulder aching, elevated CRP or ESR, morning stiffness >45 minutes) should be used to support diagnosis after excluding mimics.
- Always assess for concurrent giant cell arteritis (GCA): new-onset headache, jaw claudication, visual symptoms, or temporal artery tenderness warrant urgent temporal artery ultrasound or biopsy.
- Low-dose prednisolone (12.5–25 mg/day) is first-line therapy; expect dramatic response within 1–2 weeks — failure to respond should prompt diagnostic review.
- Taper prednisolone slowly (reduce by 2.5 mg every 2–4 weeks to 10 mg, then 1 mg every 4–8 weeks); median time to remission off steroids is 1.5–2 years.
- Relapses (up to 50–60% of patients) typically occur during taper below 7.5 mg; treat with return to the last effective dose and re-taper more slowly.
- Methotrexate (10–15 mg/week PO) is the preferred steroid-sparing agent for relapsing, refractory, or steroid-dependent PMR, or when steroid toxicity is a concern.
- Bone protection is mandatory for all patients on glucocorticoids ≥3 months: calcium, vitamin D, and alendronate or risedronate (PBS-listed for steroid-induced osteoporosis).
- Monitor CRP/ESR at each visit; disease flares usually precede symptom recurrence by weeks.
- Aboriginal and Torres Strait Islander peoples may present later, have higher rates of comorbidities affecting treatment tolerance, and experience barriers to specialist rheumatology access in remote and regional Australia.
- Exclude serious mimics before committing to long-term steroids: malignancy (myeloma, lymphoma), infection (endocarditis), thyroid disease, and calcium pyrophosphate deposition disease.
- Dual-energy X-ray absorptiometry (DEXA) should be performed at baseline and annually while on glucocorticoids; MBS item 12310 covers DEXA for patients on oral corticosteroids.
Introduction & Australian Epidemiology
Polymyalgia rheumatica (PMR) is a common, glucocorticoid-responsive inflammatory rheumatic disorder characterised by aching and morning stiffness predominantly affecting the shoulder and pelvic girdles, neck, and torso. It is the most common inflammatory rheumatic condition in Australians aged ≥50 years and frequently coexists with giant cell arteritis (GCA).
PMR primarily affects older adults, with a peak incidence between 70 and 80 years. It is rare under the age of 50. Women are affected two to three times more frequently than men. In Australia, population-based data suggest an incidence of approximately 70–100 per 100,000 person-years in those aged ≥50, comparable to Northern European cohorts. The lifetime risk for an Australian woman is approximately 2–3%.
The aetiology remains incompletely understood but involves a complex interplay of genetic susceptibility (HLA-DRB1 associations), environmental triggers (including seasonal variation with higher incidence in spring/summer in some series), immunosenescence, and pro-inflammatory cytokine pathways — particularly interleukin-6 (IL-6), tumour necrosis factor-alpha (TNF-α), and interferon-gamma. The HLA-DRB1*04 allele is shared with GCA and confers higher relapse risk.
PMR imposes a significant treatment burden: even with optimal management, most patients require 1.5 to 2 years of glucocorticoid therapy. Steroid-related adverse effects — osteoporosis, diabetes, cataracts, adrenal insufficiency, weight gain, and increased infection risk — are the major drivers of morbidity and motivate the search for steroid-sparing strategies.
Diagnosis — 2012 EULAR/ACR Classification Criteria
PMR is a clinical diagnosis supported by laboratory markers of inflammation. There is no single pathognomonic test. The 2012 EULAR/ACR classification criteria, developed for use in research and validated in Australian cohorts, provide a structured scoring framework.
Core Criteria (required for scoring)
- Age ≥50 years
- New bilateral shoulder aching
- Abnormal CRP and/or ESR
2012 EULAR/ACR Scoring Items
| Criterion | Points (without ultrasound) | Points (with ultrasound) |
|---|---|---|
| Morning stiffness duration >45 minutes | 2 | 2 |
| Hip pain or limited range of motion | 1 | 1 |
| Absence of RF and/or ACPA | 2 | 2 |
| Absence of other joint involvement | 1 | 1 |
| ≥1 shoulder with subdeltoid bursitis and/or biceps tenosynovitis and/or glenohumeral synovitis (ultrasound) | — | 1 |
| Bilateral subdeltoid bursitis, biceps tenosynovitis, or glenohumeral synovitis (ultrasound) | — | 1 |
Interpretation
- Without ultrasound: a score of ≥4 has 93% sensitivity and 78% specificity for PMR.
- With ultrasound: a score of ≥5 has 91% sensitivity and 72% specificity for PMR.
- These criteria assume that other diagnoses (infection, malignancy, inflammatory arthritis) have been excluded.
Investigations to Support Diagnosis
Key Differential Diagnoses to Exclude
| Differential | Distinguishing Features |
|---|---|
| Late-onset rheumatoid arthritis | Symmetrical small-joint synovitis, RF/ACPA may be positive, erosive changes on X-ray |
| Inflammatory myopathy (polymyositis) | Proximal weakness >pain, elevated CK, abnormal EMG/muscle biopsy |
| Multiple myeloma | Bone pain, hypercalcaemia, renal impairment, raised total protein on serum protein electrophoresis |
| Hypothyroidism | Stiffness, fatigue, weight gain; TSH and free T4 diagnostic |
| Infective endocarditis | Fever, new murmur, positive blood cultures |
| Calcium pyrophosphate deposition | Acute or chronic inflammatory arthropathy, chondrocalcinosis on X-ray |
Association with Giant Cell Arteritis
PMR and giant cell arteritis (GCA) are closely related conditions sharing overlapping immunopathology, genetic predisposition (HLA-DRB1*04), and epidemiological profiles. Approximately 40–60% of patients with GCA have coexistent PMR, while 15–30% of PMR patients harbour subclinical or overt GCA.
Screening for GCA in PMR
- Every PMR patient must be screened for GCA symptoms at initial assessment and at every follow-up visit.
- Specific enquiries: new-onset headache (especially temporal), scalp tenderness on combing, jaw claudication with chewing, visual symptoms, arm/leg claudication.
- Physical examination: palpate temporal arteries for tenderness, reduced pulse, or nodularity.
When GCA is Suspected
Implications for PMR Management
- PMR patients with concurrent GCA require higher starting doses of prednisolone (40–60 mg vs 12.5–25 mg for isolated PMR).
- Steroid taper is slower in GCA (minimum 12–24 months).
- Tocilizumab (IL-6 receptor inhibitor) is now PBS-listed for GCA in Australia (Authority Required) and may allow faster steroid tapering.
- Relapses of PMR in patients with concurrent GCA are common and may signal subclinical vasculitis flare — low threshold for re-escalation.
Steroid Therapy & Taper
Glucocorticoids remain the cornerstone of PMR therapy. An excellent response to low-dose prednisolone within 1–2 weeks is both therapeutic and diagnostic. Failure to respond should prompt diagnostic re-evaluation.
Initial Dose
Tapering Protocol
The goal is the lowest effective dose sustained for the shortest duration, balancing relapse prevention against steroid toxicity. No single taper schedule suits all patients; individualise based on disease activity and tolerability.
1. Maintain initial dose for 2–4 weeks until CRP/ESR normalise and symptoms resolve.
2. Reduce by 2.5 mg every 2 weeks (or 1 mg/month for cautious taper) until 10 mg/day.
3. Below 10 mg: reduce by 1 mg every 4–8 weeks.
4. At 5 mg: consider alternate-day dosing or further 1 mg decrements every 8 weeks.
5. Discontinue when dose is ≤2.5 mg for ≥4 weeks without relapse.
Total treatment duration: typically 12–24 months; some patients require longer.
Monitoring During Taper
- Check CRP and/or ESR at each visit (every 4–8 weeks during taper, more frequently in early treatment).
- Rising inflammatory markers often precede symptom relapse by 2–4 weeks — consider slowing the taper.
- Monitor blood pressure, glucose (HbA1c every 3–6 months), weight, and symptoms of steroid toxicity.
- Screen for adrenal insufficiency symptoms (fatigue, nausea, hypotension) as dose approaches physiologic replacement (5–7.5 mg/day).
- If adrenal insufficiency suspected: morning cortisol or short Synacthen test. Do not stop prednisolone abruptly.
Steroid Side Effects
| System | Adverse Effects | Monitoring |
|---|---|---|
| Musculoskeletal | Osteoporosis, avascular necrosis, proximal myopathy | DEXA at baseline and annually; FRAX score |
| Metabolic | Diabetes, weight gain, dyslipidaemia | Fasting glucose at baseline, then 3-monthly; HbA1c |
| Ophthalmological | Posterior subcapsular cataracts, glaucoma | Annual ophthalmology review if >7.5 mg >6 months |
| Cardiovascular | Hypertension, fluid retention | BP at each visit |
| Infectious | Increased risk of infection, reactivation of latent TB | Consider TB screening (IGRA) at baseline |
| Dermatological | Skin fragility, bruising, striae | Clinical assessment |
| Psychiatric | Insomnia, mood changes, psychosis (rare) | Patient enquiry at each visit |
Steroid-Sparing Agents
Not all PMR patients require steroid-sparing agents. However, they should be considered early in patients who relapse during taper, require prolonged moderate-dose steroids (≥7.5 mg prednisolone for ≥6 months), or have significant steroid-related comorbidities (diabetes, osteoporosis, glaucoma).
Methotrexate — First-Line Steroid Sparer
Other Steroid-Sparing Options
• Relapse during first steroid taper
• Prednisolone dose ≥7.5 mg/day required for >6 months
• Steroid-related adverse effects: new diabetes, fracture, cataracts, significant weight gain
• Pre-existing comorbidity exacerbated by steroids (diabetes, osteoporosis, glaucoma)
• Patient preference after discussion of risks/benefits
Agents NOT Recommended
- NSAIDs alone: Inadequate for PMR; may be used adjunctively for mild symptoms during taper.
- TNF inhibitors (infliximab, etanercept, adalimumab): Trials in PMR have been negative or inconclusive; not recommended.
- Azathioprine: Insufficient evidence; not standard of care for PMR.
Bone Protection
Glucocorticoid-induced osteoporosis (GIOP) is a major concern in PMR patients, who are already elderly and often have age-related bone loss. All patients commencing prednisolone ≥3 months require bone-protective measures. Australian guidelines (RACGP, Osteoporosis Australia) recommend risk stratification and prophylaxis.
Risk Assessment
- Perform FRAX® score calculation (adjusted for glucocorticoid dose) at baseline.
- DEXA scan at commencement of glucocorticoids (MBS item 12310) and annually while on treatment.
- Consider bone protection for all patients aged ≥70 or those with prior fragility fracture — these patients are automatically high-risk.
Universal Bone Protection Measures
High-Risk Patients — Additional Options
- Zoledronic acid (Aclasta®): 5 mg IV once yearly. PBS-listed for osteoporosis (Authority Required in some indications). Useful when oral bisphosphonates are not tolerated or compliance is a concern. Contraindicated if eGFR <35 mL/min/1.73 m².
- Denosumab (Prolia®): 60 mg SC every 6 months. PBS Authority Required for severe osteoporosis. Can be used in renal impairment (unlike bisphosphonates). Monitor calcium closely; rebound vertebral fractures may occur on discontinuation.
Atypical & Relapsing PMR
Relapse
Relapse is common in PMR, affecting 50–60% of patients during or after glucocorticoid taper. Relapse is defined as recurrence of PMR symptoms with or without elevated inflammatory markers while on or after stopping glucocorticoids.
Features Suggesting Relapse
- Recurrence of bilateral shoulder and/or hip girdle aching and stiffness.
- Rising CRP and/or ESR (often precedes symptoms by 2–4 weeks).
- Fatigue, malaise, and reduced function.
- Typically occurs when prednisolone is tapered below 7.5 mg/day or after cessation.
Management of Relapse
Atypical Presentations
A minority of patients present with atypical features that can complicate diagnosis or suggest an alternative diagnosis.
| Atypical Feature | Consideration |
|---|---|
| Peripheral arthritis (hands, wrists, knees) | Consider late-onset rheumatoid arthritis (LORA), remitting seronegative symmetrical synovitis with pitting oedema (RS3PE), or overlap syndrome |
| Normal ESR and CRP | Seen in ~5% of PMR. Do not exclude diagnosis. Consider occult malignancy, fibromyalgia, or statin myopathy. |
| Distal swelling with pitting oedema | RS3PE syndrome (remitting seronegative symmetrical synovitis with pitting oedema) — responds to low-dose steroids, may be PMR variant |
| Onset <50 years | PMR extremely rare <50; strongly consider alternative diagnoses including malignancy and inflammatory arthritis |
| Poor steroid response | Re-evaluate diagnosis. Consider myeloma, hypothyroidism, malignancy, fibromyalgia, or corticosteroid myopathy causing apparent relapse |
| Systemic features (fever, weight loss, night sweats) | Consider occult malignancy (lymphoma, myeloma), infection (endocarditis), or concurrent GCA |
Steroid-Resistant or Steroid-Dependent PMR
- Definition: Failure to reduce prednisolone below 10 mg/day without relapse after two attempts, or inability to discontinue after 2 years.
- Re-evaluate the diagnosis thoroughly — perform imaging, consider malignancy screen, and assess for concurrent GCA.
- Initiate methotrexate if not already commenced. Leflunomide as second-line.
- Consider tocilizumab in specialist centres for refractory cases (off-label for PMR; PBS-authorised for GCA).
- Refer to rheumatology if not already under specialist care.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples may experience PMR differently due to higher background rates of comorbid chronic disease, barriers to specialist access, and the impact of racism and social disadvantage on healthcare engagement. Culturally safe, patient-centred care is essential.
Quick Reference — PMR Management at a Glance
📚 References
- 1. Dasgupta B, Cimmino MA, Maradit-Kremers H, et al. 2012 provisional classification criteria for polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Ann Rheum Dis. 2012;71(4):484–492.
- 2. Dejaco C, Singh YP, Perel P, et al. 2015 recommendations for the management of polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology task force collaborative initiative. Arthritis Rheumatol. 2015;67(10):2569–2580.
- 3. Buttgereit F, Dejaco C, Matteson EL, Dasgupta B. Polymyalgia rheumatica and giant cell arteritis: a systematic review. JAMA. 2016;315(22):2442–2458.
- 4. Caporali R, Cimmino MA, Ferraccioli G, et al. Prednisone plus methotrexate for polymyalgia rheumatica: a randomized, double-blind, placebo-controlled trial. Ann Intern Med. 2004;141(7):493–500.
- 5. Bonelli M, Radner H, Kerschbaumer A, et al. Tocilizumab in patients with new onset polymyalgia rheumatica (PMR-SPARE): a phase 2/3 randomised controlled trial. Ann Rheum Dis. 2022;81(6):831–837.
- 6. Australian Institute of Health and Welfare (AIHW). Rheumatic and musculoskeletal disease in Aboriginal and Torres Strait Islander peoples. AIHW, Canberra; 2019.
- 7. Royal Australian College of General Practitioners (RACGP). Recommended guidelines for the management of glucocorticoid-induced osteoporosis. RACGP, Melbourne; 2017.
- 8. Kermani TA, Warrington KJ, Cuthbertson D, et al. Disease relapses among patients with giant cell arteritis: a prospective, longitudinal cohort study. J Rheumatol. 2015;42(7):1213–1217.
- 9. Department of Health and Aged Care. Schedule of Pharmaceutical Benefits. Commonwealth of Australia, Canberra. Available at: pbs.gov.au. Accessed 2025.
- 10. Cimmino MA, Zaccaria A. Epidemiology of polymyalgia rheumatica. Clin Exp Rheumatol. 2000;18(4 Suppl 20):S9–S11.
- 11. Gonzalez-Gay MA, Vazquez-Rodriguez TR, Lopez-Diaz MJ, et al. Epidemiology of giant cell arteritis and polymyalgia rheumatica. Arthritis Care Res. 2009;61(10):1454–1461.
- 12. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 2nd edn. Menzies School of Health Research, Darwin; 2020. [Referenced for remote and Indigenous health service delivery models.]