📋 Key Information Summary
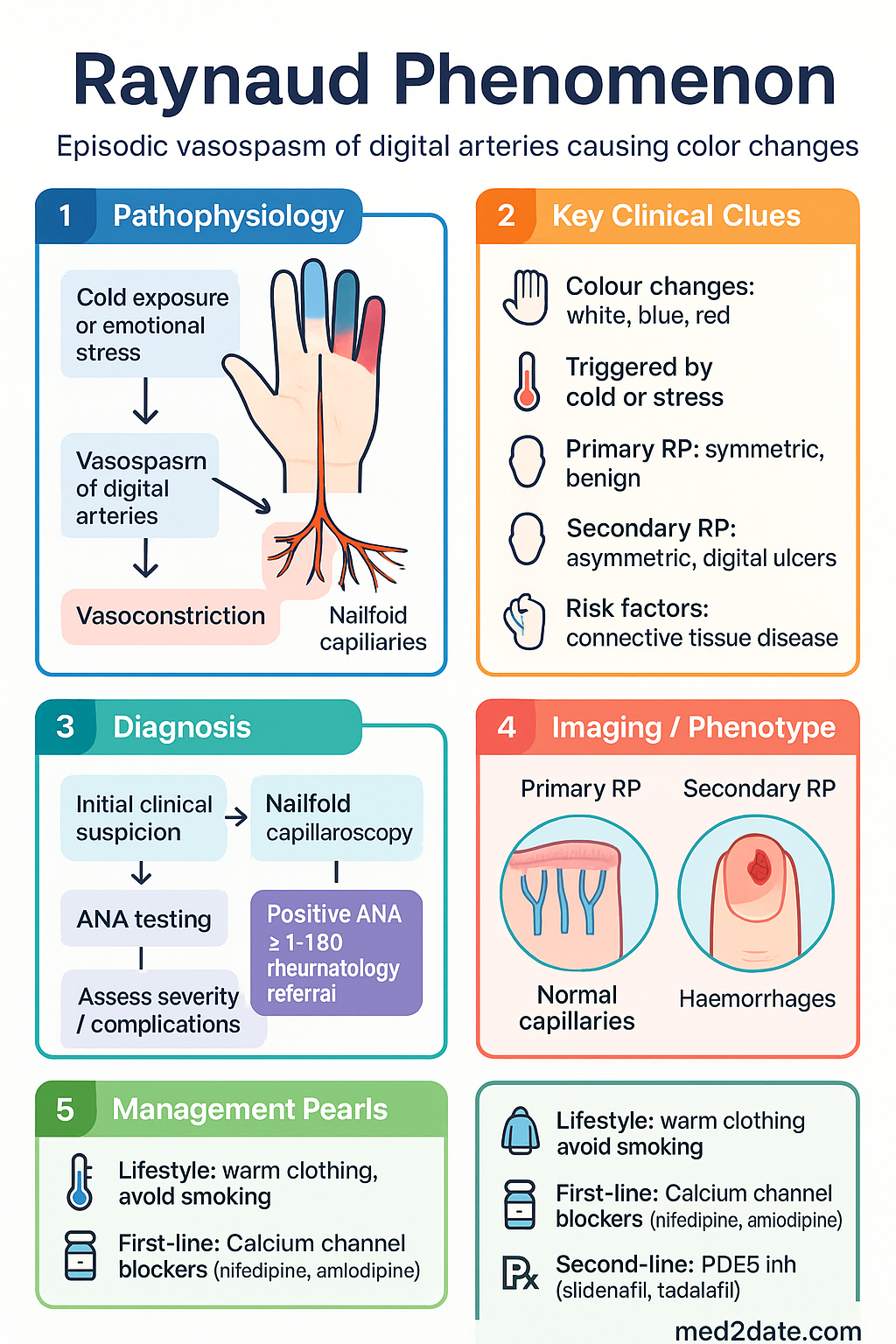
- Raynaud phenomenon (RP) is episodic vasospasm of digital arteries causing colour changes (white → blue → red) triggered by cold or emotional stress; prevalence ~3–5% in Australia.
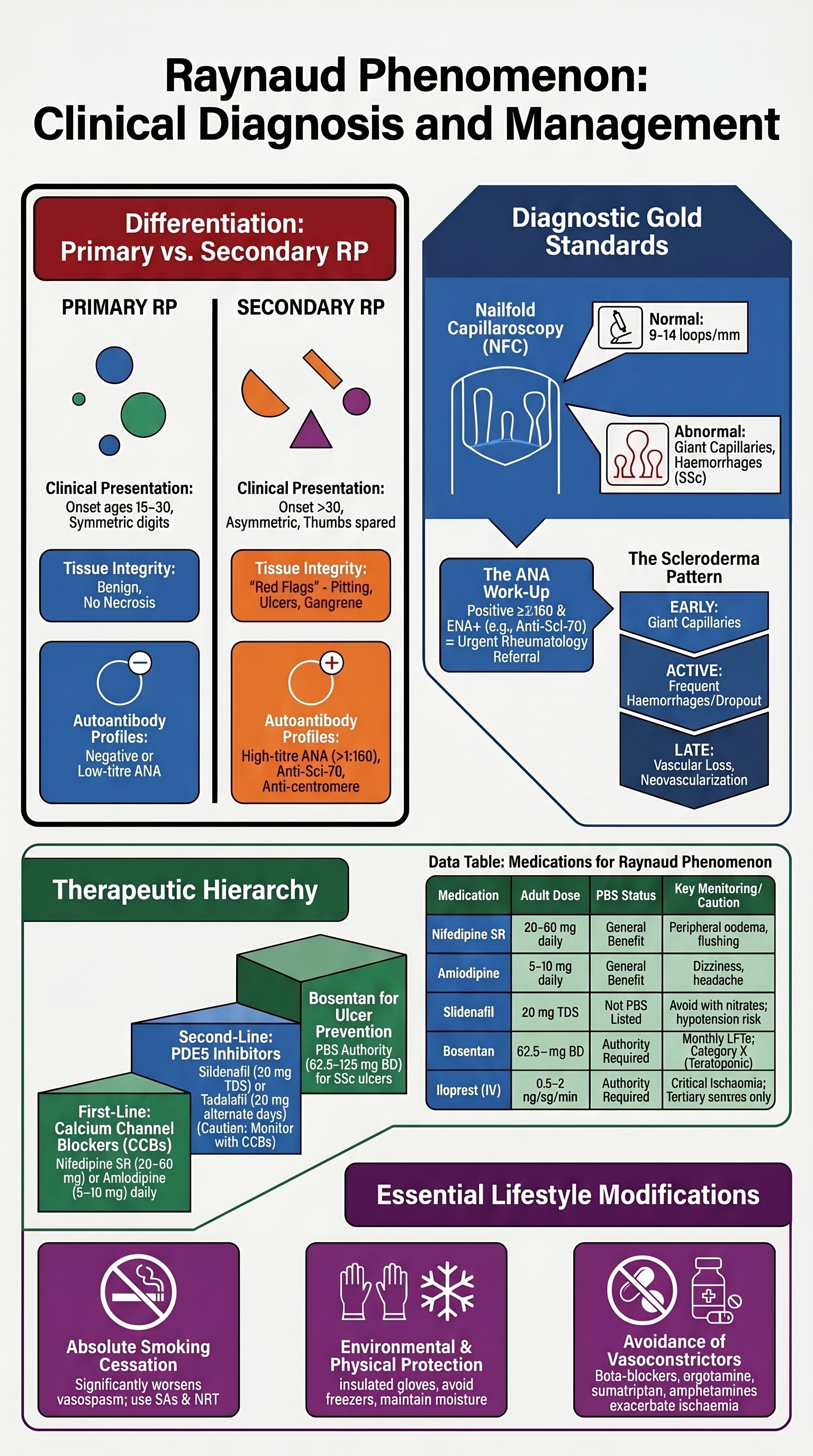
- Primary RP (Raynaud disease) is benign, symmetric, with no tissue necrosis, negative autoantibodies, and normal nailfold capillaries — accounts for ~80–90% of cases.
- Secondary RP is associated with connective tissue disease (especially systemic sclerosis), has asymmetric onset, digital pitting/ulcers, abnormal nailfold capillaries, and positive ANA/anti-centromere/anti-Scl-70 antibodies.
- Nailfold capillaroscopy is the single most important investigation to differentiate primary from secondary RP — giant capillaries and haemorrhages indicate early systemic sclerosis.
- ANA testing is recommended for all RP patients; a positive ANA >1:160 with specific extractable nuclear antigens (anti-centromere, anti-Scl-70, anti-RNA polymerase III) warrants rheumatology referral.
- First-line pharmacotherapy for symptomatic RP is a dihydropyridine calcium channel blocker — nifedipine slow-release 20–60 mg daily or amlodipine 5–10 mg daily.
- Sildenafil 20 mg TDS or tadalafil 20 mg on alternate days is second-line therapy when CCBs are ineffective or not tolerated; neither is PBS-listed for RP.
- Digital ulcers occur in ~30% of systemic sclerosis patients; bosentan 62.5 mg BD (increasing to 125 mg BD) is PBS Authority Required for prevention of new digital ulcers in scleroderma.
- Lifestyle measures (smoking cessation, warm clothing, avoiding vasoconstrictive drugs, hand-warmers) are essential in all patients and may be sufficient for mild primary RP.
- Aboriginal and Torres Strait Islander peoples may have higher prevalence of autoimmune conditions contributing to secondary RP; remote access to rheumatology and capillaroscopy is limited — telehealth and RFDS referral pathways should be used.
- Emergency IV iloprost infusion is indicated for critical digital ischaemia with threatened gangrene — available at major tertiary centres.
- Avoid β-blockers, ergotamine, sumatriptan, clonidine, and amphetamines in all RP patients as these worsen vasospasm.
Introduction & Australian Epidemiology
Raynaud phenomenon (RP) is a reversible vasospastic disorder of the digital arteries and cutaneous microcirculation, characterised by episodic colour changes of the digits — typically pallor (white), followed by cyanosis (blue) and reactive hyperaemia (red) — provoked by cold exposure or emotional stress. The condition may be primary (idiopathic, benign) or secondary to an underlying disease, most commonly a connective tissue disorder.
In Australia, primary RP affects approximately 3–5% of the general population, with a higher prevalence in women (female-to-male ratio ~4:1), young adults aged 15–30 years, and those with a family history. Secondary RP is estimated to affect 0.5–1% of the population and is most frequently associated with systemic sclerosis (scleroderma), where it is present in >95% of cases. The Australian Scleroderma Cohort Study has documented that digital ulcers — a serious complication of secondary RP — occur in approximately 30% of systemic sclerosis patients and are associated with significant morbidity including pain, infection, and digital amputation.
Cold ambient temperatures in southern Australian states (Victoria, Tasmania, South Australia) exacerbate symptoms. Primary RP is generally self-limiting and does not progress to tissue injury, whereas secondary RP may lead to digital pitting, ulceration, gangrene, and auto-amputation. Correct classification is therefore critical to guide investigation, treatment, and follow-up.
Primary vs Secondary Raynaud
Distinguishing primary from secondary RP is the cornerstone of management. Primary RP (Raynaud disease) is a benign vasospastic condition without underlying pathology, while secondary RP (Raynaud syndrome/phenomenon) is a manifestation of another disease — most commonly a connective tissue disease.
| Feature | Primary RP | Secondary RP |
|---|---|---|
| Age of onset | 15–30 years | >30 years (variable) |
| Sex | Female >> Male (4:1) | Depends on underlying disease |
| Symmetry | Symmetric, all digits | Often asymmetric, may spare thumbs |
| Tissue necrosis | Never | Digital pitting, ulcers, gangrene |
| Nailfold capillaries | Normal | Abnormal (giant capillaries, haemorrhages) |
| ANA | Negative or low-titre | Often positive (>1:160) |
| Specific autoantibodies | Absent | Anti-centromere, anti-Scl-70, anti-RNA Pol III |
| ESR / inflammatory markers | Normal | May be elevated |
| Associated features | None | Skin tightening, arthritis, sicca, dysphagia, ILD |
Risk factors for progression from primary to secondary RP include a positive ANA at baseline, abnormal nailfold capillaroscopy, and older age at onset. Longitudinal studies suggest approximately 10–15% of patients initially diagnosed with primary RP will develop features of a connective tissue disease over 10 years of follow-up.
Nailfold Capillaroscopy
Nailfold capillaroscopy (NFC) is the gold-standard bedside and specialist investigation for differentiating primary from secondary RP. It examines the microvascular architecture at the nailfold — the area where cutaneous capillary loops are visible — using a handheld dermatoscope, ophthalmoscope, or stereomicroscope.
Technique
- Examine at least 8 fingers (exclude thumbs which have anatomical variation).
- Apply a drop of immersion oil or gel to the nailfold to improve optical contact.
- Use ×200 magnification (stereomicroscope) for detailed assessment or a dermatoscope/USB videocapillaroscope for clinic-based screening.
- Allow the patient to acclimatise to room temperature for 15–20 minutes before examination.
Normal (Primary RP) Findings
- Regular, homogenous capillary loops arranged in parallel rows.
- No capillary enlargement, haemorrhages, or dropout.
- Normal capillary density: 9–14 loops per mm.
Abnormal (Secondary RP — Scleroderma Pattern) Findings
Vasodilator Therapy (CCBs, Sildenafil)
Pharmacotherapy is indicated when lifestyle measures are insufficient to control RP symptoms, particularly when attacks are frequent, prolonged, or interfere with daily activities and work. All patients with secondary RP and digital ischaemia should receive vasodilator therapy.
First-Line: Dihydropyridine Calcium Channel Blockers
Common adverse effects include peripheral oedema, headache, flushing, and dizziness. These are dose-dependent and more common with nifedipine than amlodipine. Sustained-release formulations reduce the incidence of adverse effects. A trial of at least 4 weeks at optimal dose is recommended before determining efficacy.
Second-Line: PDE5 Inhibitors
Other Vasodilator Options (Less Commonly Used)
| Agent | Class | Dose | PBS |
|---|---|---|---|
| Losartan | ARB | 25–50 mg PO daily | General Benefit |
| Fluoxetine | SSRI | 20 mg PO daily | General Benefit |
| Atorvastatin | Statin (pleiotropic) | 40 mg PO daily (investigational) | General Benefit |
| Iloprost (IV) | Prostacyclin analogue | 0.5–2 ng/kg/min IV infusion over 6 hours × 3–5 days | Authority Required |
IV iloprost is reserved for critical digital ischaemia with threatened gangrene and is available at major tertiary rheumatology centres in Australia. Continuous cardiac monitoring is required during infusion due to risk of hypotension and tachycardia.
Digital Ulcers & Bosentan
Digital ulcers are a major complication of secondary RP, occurring in approximately 30% of patients with systemic sclerosis. They result from intimal proliferation, thrombosis, and ischaemia of digital arteries, often complicated by infection. Digital ulcers cause severe pain, functional impairment, and may lead to osteomyelitis, gangrene, and auto-amputation.
Classification of Digital Lesions
| Type | Description | Management |
|---|---|---|
| Digital pitting | Small depressions at fingertips from healed ulcers | Vasodilators, skin care |
| Ischaemic digital ulcer | Punched-out lesion with pale or necrotic base on finger pad or periungual area | Vasodilators, wound care, consider bosentan/IV iloprost |
| Calcific ulcer | Ulcer overlying calcinosis deposits | Surgical debridement, CO₂ laser, topical sodium thiosulfate |
| Gangrene | Tissue necrosis — dry or wet | IV iloprost, antibiotics, surgical review |
Bosentan for Digital Ulcer Prevention
Wound Care for Digital Ulcers
- Maintain moisture balance — hydrocolloid or foam dressings for clean ulcers.
- Debride necrotic tissue; consider surgical debridement for calcinosis-related ulcers.
- Swab for culture and sensitivity if signs of infection (erythema, purulence, warmth).
- Empirical antibiotics for infected digital ulcers: flucloxacillin 500 mg PO QDS (or cephalexin 500 mg PO QDS if penicillin allergy) — cover S. aureus.
- If MRSA suspected or confirmed: doxycycline 100 mg PO BD or TMP-SMX DS PO BD.
- Refer to hand surgery/plastic surgery for threatened gangrene or non-healing ulcers.
ANA & Autoantibody Work-Up
Antinuclear antibody (ANA) testing is recommended for all patients presenting with RP to screen for underlying connective tissue disease. The pattern and titre of ANA, combined with extractable nuclear antigen (ENA) profiling, help risk-stratify patients and guide rheumatology referral.
Recommended Work-Up
Autoantibody–Disease Associations
| Antibody | Associated Condition | Clinical Significance |
|---|---|---|
| Anti-centromere (ACA) | Limited cutaneous SSc (CREST) | Higher risk of pulmonary arterial hypertension (PAH); generally slower progression |
| Anti-Scl-70 (Topo I) | Diffuse cutaneous SSc | Higher risk of interstitial lung disease (ILD); worse prognosis |
| Anti-RNA Pol III | Diffuse cutaneous SSc | Rapid skin thickening; increased risk of scleroderma renal crisis |
| Anti-U1 RNP | Mixed connective tissue disease | Overlap features of SSc, SLE, polymyositis |
| Anti-Ro (SSA) / Anti-La (SSB) | Sjögren syndrome, SLE | Sicca symptoms; neonatal lupus if anti-Ro positive in pregnancy |
| Anti-Smith, anti-dsDNA | Systemic lupus erythematosus | Lupus-specific; dsDNA correlates with nephritis activity |
Lifestyle Measures
Lifestyle modifications are the cornerstone of RP management for all patients — both primary and secondary. These measures reduce attack frequency and severity and may be sufficient alone for mild primary RP.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Wigley FM, Flavahan NA. Raynaud's phenomenon. N Engl J Med. 2016;375(6):556–565.
- 2. Hughes M, Herrick AL. Raynaud's phenomenon. Best Pract Res Clin Rheumatol. 2016;30(1):112–132.
- 3. Cutolo M, Herrick AL, Distler O, et al. Nailfold videocapillaroscopic features and other clinical risk factors for digital ulcers in systemic sclerosis: a multicentre, prospective cohort study. Ann Rheum Dis. 2016;75(9):1633–1638.
- 4. Herrick AL, Cutolo M. Clinical implications from capillaroscopic analysis in patients with Raynaud's phenomenon and systemic sclerosis. Arthritis Rheum. 2013;65(10):2515–2523.
- 5. Rirash F, Tingey PC, Harding SE, et al. Calcium channel blockers for primary and secondary Raynaud's phenomenon. Cochrane Database Syst Rev. 2017;12:CD000467.
- 6. Roustit M, Blaise S, Allanore Y, et al. Phosphodiesterase-5 inhibitors for the treatment of secondary Raynaud's phenomenon: systematic review and meta-analysis of randomised trials. Ann Rheum Dis. 2013;72(10):1696–1699.
- 7. Matucci-Cerinic M, Denton CP, Furst DE, et al. Bosentan treatment of digital ulcers related to systemic sclerosis: results from the RAPIDS-2 randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. 2011;70(1):32–38.
- 8. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2023 summary report. Canberra: AIHW; 2023.
- 9. Nikpour M, Hissaria P, Byron J, et al. Prevalence, correlates and clinical usefulness of antibodies to RNA polymerase III in systemic sclerosis: a cross-sectional analysis of data from an Australian cohort. Arthritis Res Ther. 2011;13(6):R211.
- 10. Khanna D, Gladue H, Channick R, et al. Recommendations for screening and detection of connective tissue disease-associated pulmonary arterial hypertension (CTD-PAH). Arthritis Rheum. 2013;65(2):549–557.
- 11. National Health and Medical Research Council (NHMRC). Australian guidelines to reduce health risks from drinking alcohol. Canberra: NHMRC; 2020.
- 12. Belch JJ, Carlizza A, Carpentier PH, et al. Recommendations for the management of Raynaud's phenomenon. Vasa. 2017;46(Suppl 95):1–22.
- 13. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.