📋 Key Information Summary
- Gastric adenocarcinoma is the fifth most common cancer in Australia, with ~2,500 new cases diagnosed annually and a 5-year survival rate of approximately 30%.
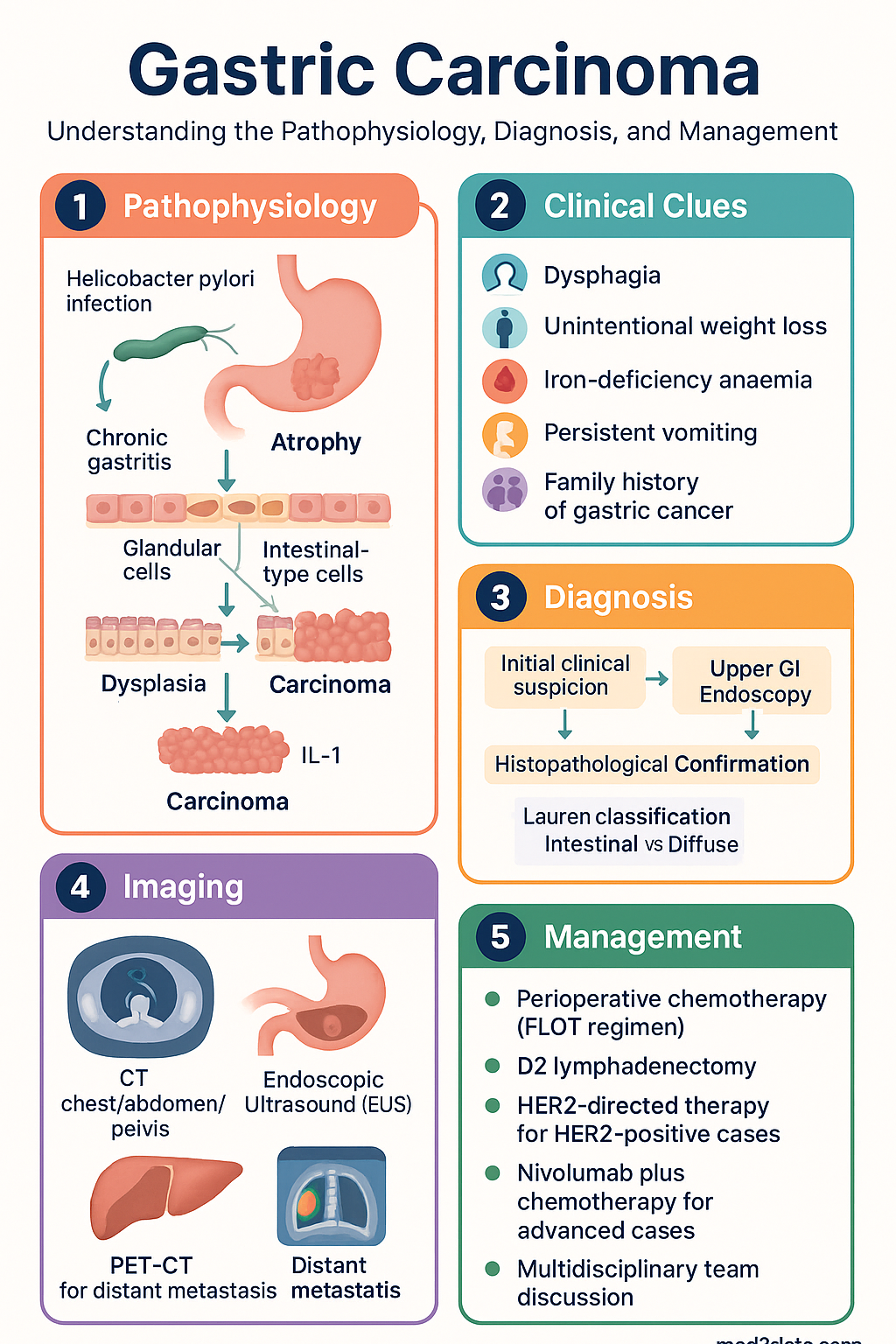
- Risk factors include Helicobacter pylori infection, tobacco smoking, high-salt diet, family history, gastric atrophy, and intestinal metaplasia.
- Lauren classification (intestinal vs diffuse) and WHO histological classification remain the primary pathological frameworks guiding prognosis and treatment.
- Early-stage disease is often asymptomatic; alarm features (dysphagia, unintentional weight loss, iron-deficiency anaemia, persistent vomiting) warrant urgent upper GI endoscopy.
- CT staging (chest/abdomen/pelvis), endoscopic ultrasound (EUS), and PET-CT form the staging triad; laparoscopy with peritoneal lavage is recommended for stage II–III disease to detect occult peritoneal metastasis.
- Perioperative chemotherapy (FLOT regimen: 5-fluorouracil, leucovorin, oxaliplatin, docetaxel) is the standard of care for resectable locally advanced (cT2 or N+) gastric adenocarcinoma in fit patients.
- D2 lymphadenectomy is the recommended surgical standard in Australian centres; R0 resection is the primary surgical goal.
- Adjuvant capecitabine plus oxaliplatin (CAPOX) or S-1 is used post-operatively when pre-operative chemotherapy was not given; HER2-directed therapy (trastuzumab) is first-line for HER2-positive metastatic disease.
- Nivolumab plus chemotherapy is approved first-line for advanced/metastatic gastric cancer regardless of PD-L1 status in Australia (PBS-listed).
- Molecular profiling (HER2, microsatellite instability [MSI], PD-L1, Claudin 18.2) is now essential for all advanced-stage cases to guide targeted and immunotherapy.
- Aboriginal and Torres Strait Islander peoples experience higher rates of H. pylori infection and later-stage presentation; culturally safe, community-based screening programmes are critical.
- Multidisciplinary team (MDT) discussion at a designated cancer centre is mandatory for all cases, ideally prior to any treatment decisions.
Introduction & Australian Epidemiology
Gastric carcinoma is a malignant epithelial neoplasm of the stomach, with adenocarcinoma accounting for over 90% of all gastric malignancies. Despite declining global incidence, gastric cancer remains a significant cause of cancer-related mortality in Australia due to late-stage presentation and the aggressive biology of certain subtypes.
In Australia, approximately 2,500 new cases of gastric cancer are diagnosed each year, with an age-standardised incidence of approximately 7.9 per 100,000 population. The median age at diagnosis is 70 years, and males are affected approximately twice as frequently as females. The 5-year overall survival remains poor at approximately 30%, reflecting the fact that the majority of patients present with locally advanced or metastatic disease.
Geographic and ethnic variation in incidence is notable. Higher rates are observed in East Asian countries, and within Australia, individuals of East Asian, Eastern European, and South American descent carry elevated risk. The incidence in Aboriginal and Torres Strait Islander peoples is comparable to or slightly higher than the non-Indigenous population, but outcomes are significantly worse owing to later diagnosis, comorbidity burden, and barriers to timely healthcare access.
The anatomical distribution of gastric adenocarcinoma has shifted over recent decades, with an increase in proximal (cardia and gastro-oesophageal junction) tumours in Western countries, including Australia, contrasting with the traditionally more common distal (antral/pyloric) predominance seen in high-incidence regions and in association with H. pylori infection.
Epidemiology & Risk Factors
Key Risk Factors
| Risk Factor | Relative Risk | Mechanism / Notes |
|---|---|---|
| Helicobacter pylori infection | 2–6× | Chronic gastritis → atrophy → intestinal metaplasia → dysplasia → carcinoma (Correa cascade). CagA-positive strains carry highest risk. |
| Chronic atrophic gastritis / intestinal metaplasia | 6–10× | Surveillance endoscopy every 3 years recommended for extensive metaplasia (MAPS II guidelines). |
| Tobacco smoking | 1.5–2× | Dose-dependent risk; cessation reduces risk over 10–15 years. |
| Family history (first-degree relative) | 2–3× | Higher if relative diagnosed <50 years. Consider hereditary diffuse gastric cancer (CDH1 mutation). |
| Hereditary diffuse gastric cancer (HDGC) | Very high | CDH1 pathogenic variant; prophylactic gastrectomy recommended by age 20–30. |
| High-salt diet / processed meat / nitrosamines | 1.5–2× | Promotes mucosal inflammation and H. pylori colonisation. |
| Low fruit and vegetable intake | 1.5–2× | Reduced antioxidant defence and vitamin C intake. |
| Pernicious anaemia / autoimmune gastritis | 2–4× | Risk of type 1 gastric neuroendocrine tumour and adenocarcinoma. |
| Prior gastric surgery (>15 years) | 2–4× | Stump carcinoma following partial gastrectomy (Billroth II > Billroth I). |
| Epstein-Barr virus (EBV) | Variable | ~10% of gastric adenocarcinomas are EBV-positive; associated with PIK3CA mutations and favourable immunotherapy response. |
Protective Factors
- Diets rich in fresh fruit and vegetables
- Successful H. pylori eradication (reduces risk by ~34% in meta-analyses)
- Non-smoking status
- Regular aspirin / NSAID use (modest risk reduction; not recommended solely for this indication)
Pathology & Classification
Lauren Classification
| Type | Frequency | Features | Association |
|---|---|---|---|
| Intestinal | ~50–60% | Gland-forming, cohesive tumour cells; resembles intestinal epithelium | H. pylori, atrophic gastritis, environmental factors, older age, male predominance |
| Diffuse | ~30–40% | Non-cohesive, signet-ring cells; infiltrates submucosally; poor differentiation | Younger patients, CDH1 mutation, E-cadherin loss, worse prognosis |
| Mixed / Indeterminate | ~10% | Features of both types | Variable prognosis |
WHO Histological Classification
- Tubular adenocarcinoma
- Papillary adenocarcinoma
- Mucinous adenocarcinoma
- Poorly cohesive carcinoma (including signet-ring cell carcinoma)
- Mixed carcinoma
Molecular Subtypes (TCGA Classification)
The Cancer Genome Atlas (TCGA) project identified four molecular subtypes of gastric adenocarcinoma, increasingly used to guide therapy:
| Subtype | Frequency | Key Features | Therapeutic Implications |
|---|---|---|---|
| EBV-positive | ~10% | PIK3CA mutations, PD-L1/2 amplification, high CpG island methylation | Favourable response to immune checkpoint inhibitors (ICI) |
| Microsatellite instability–high (MSI-H) | ~20% | MLH1 promoter hypermethylation, high tumour mutational burden | Best ICI response; avoid 5-FU in some contexts; better prognosis |
| Genomically stable (GS) | ~20% | Diffuse histology, CDH1 and RHOA mutations | Potential targets: CLDN18.2 (zolbetuximab), FGFR2 |
| Chromosomal instability (CIN) | ~50% | TP53 mutations, RTK/RAS amplification (HER2, EGFR, MET) | HER2-targeted therapy (trastuzumab); anti-VEGFR (ramucirumab) |
Borrmann Macroscopic Classification
- Type I: Polypoid / fungating
- Type II: Ulcerated with raised margins
- Type III: Ulcerated with infiltrative margins (most common)
- Type IV: Diffusely infiltrative (linitis plastica) — worst prognosis
Clinical Features & Diagnosis
Presenting Features
Early gastric cancer is frequently asymptomatic or produces only non-specific dyspeptic symptoms, contributing to late diagnosis. The following alarm features should prompt urgent investigation in patients aged ≥50 years or those with risk factors:
| Symptom | Frequency at Diagnosis | Clinical Note |
|---|---|---|
| Epigastric pain / discomfort | ~70% | Often initially responsive to PPI, causing diagnostic delay |
| Weight loss | ~60% | Strong predictor of advanced disease |
| Nausea / vomiting | ~50% | Suggests gastric outlet obstruction if proximal/distal tumour |
| Dysphagia | ~25% | Indicates proximal / cardia involvement |
| GI bleeding (melaena / haematemesis) | ~20% | May cause iron-deficiency anaemia |
| Early satiety | ~15% | Suggests reduced gastric compliance / linitis plastica |
Paraneoplastic Syndromes
- Dermatomyositis / acanthosis nigricans: may be presenting feature
- Virchow's node: left supraclavicular lymphadenopathy (Troisier sign)
- Sister Mary Joseph nodule: periumbilical metastatic deposit
- Krukenberg tumour: ovarian metastasis with signet-ring cells
- Irish node: left axillary lymphadenopathy
- Mikulicz syndrome: lacrimal and salivary gland enlargement (rare)
Diagnostic Pathway
Investigations
Staging & Management
AJCC / UICC TNM Staging (8th Edition)
| Stage | TNM | 5-Year Survival (Approx.) | Primary Management |
|---|---|---|---|
| I | T1N0M0 | ~90% | Endoscopic resection (EMR/ESD) if criteria met; or surgery (D1+ lymphadenectomy) |
| II | T1N1–2 / T2N0–1 / T3N0M0 | ~60–70% | Perioperative chemotherapy (FLOT) → D2 gastrectomy |
| III | T2N2 / T3N1–2 / T4a–bN0–2M0 | ~20–45% | Perioperative chemotherapy (FLOT) → D2 gastrectomy; adjuvant chemo if pre-op not given |
| IV | Any T, Any N, M1 | ~5–10% | Systemic palliative chemotherapy; molecular-guided targeted/immunotherapy |
Early Gastric Cancer — Endoscopic Resection Criteria
- Differentiated-type, mucosal cancer, no ulceration, any size
- Differentiated-type, mucosal cancer, ulceration, ≤30 mm
- Undifferentiated-type, mucosal cancer, no ulceration, ≤20 mm
- SM1 invasion (≤500 μm submucosal), differentiated-type, no lymphovascular invasion
ESD should be performed at experienced tertiary centres. If curative criteria not met, surgical gastrectomy with D1+ lymphadenectomy is recommended.
Perioperative Chemotherapy — Standard of Care
Adjuvant Chemotherapy (when pre-operative therapy not given)
Surgery — D2 Lymphadenectomy
D2 gastrectomy (removal of level 1 and 2 lymph nodes) is the recommended surgical standard in Australia, performed at high-volume centres. Key principles include:
- Goal: R0 (microscopically negative) resection with ≥16 lymph nodes harvested
- Total gastrectomy: For proximal tumours, tumours crossing the incisura, or diffuse-type (signet-ring) cancers
- Distal subtotal gastrectomy: For distal tumours with adequate proximal margin (≥5 cm intestinal / ≥8 cm diffuse)
- Roux-en-Y reconstruction: Preferred after total gastrectomy to minimise reflux
- Minimally invasive approach: Laparoscopic gastrectomy equivalent outcomes at experienced centres; robotic surgery increasingly available
Metastatic Disease — First-Line Systemic Therapy
First-line treatment of metastatic gastric adenocarcinoma is guided by molecular profiling. All patients should have HER2, MSI/dMMR, and PD-L1 testing.
Metastatic Disease — Subsequent Lines
Monitoring & Follow-Up
Post-Surgical Surveillance (Resected Disease)
| Timepoint | Investigations | Purpose |
|---|---|---|
| Every 3–6 months × 2 years | Clinical review, FBC, LFTs, CEA, CA 19-9, CT CAP q6–12m | Early recurrence detection |
| Every 6–12 months, years 3–5 | Clinical review, tumour markers, CT if symptoms | Late recurrence surveillance |
| After 5 years | Annual clinical review; imaging if symptomatic | Long-term survivorship care |
| Post-gastrectomy (ongoing) | Vitamin B12, iron studies, calcium, vitamin D q6–12m | Nutritional deficiency monitoring (B12, iron, calcium) |
Nutritional Support Post-Gastrectomy
- Dumping syndrome: Small, frequent meals; avoid simple carbohydrates; complex carbohydrate–rich snacks
- Vitamin B12: Lifelong supplementation — cyanocobalamin 1,000 μg IM monthly (or 100 μg SC every 2–3 months) if total gastrectomy; monitor levels annually
- Iron: Ferrous fumarate 200 mg PO BD; IV iron (ferric carboxymaltose) if intolerant of oral
- Calcium + Vitamin D: Calcium carbonate 1.2 g PO daily + cholecalciferol 1,000 IU PO daily; DEXA scan at baseline and q2 years
- Dietitian referral: All patients post-gastrectomy should receive specialist dietitian input
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Cancer Australia. Gastric cancer in Australia statistics. Sydney: Cancer Australia; 2024. Available from: cancer.gov.au.
- 2. Al-Batran S-E, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948-1957.
- 3. Janjigian YY, Shitara K, Moehler M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial. Lancet. 2021;398(10294):27-40.
- 4. Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376(9742):687-697.
- 5. Shitara K, Bang YJ, Iwasa S, et al. Trastuzumab deruxtecan in previously treated HER2-positive gastric cancer. N Engl J Med. 2020;382(25):2419-2430.
- 6. Shah MA, Shitara K, Ajani JA, et al. Zolbetuximab plus CAPOX in CLDN18.2-positive gastric or gastroesophageal junction adenocarcinoma: the randomized, phase 3 GLOW trial. Nat Med. 2023;29(8):2133-2141.
- 7. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2021 (6th edition). Gastric Cancer. 2023;26(1):1-25.
- 8. Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature. 2014;513(7517):202-209.
- 9. Ford AC, Yuan Y, Moayyedi P. Helicobacter pylori eradication therapy to prevent gastric cancer: systematic review and meta-analysis. Gut. 2020;69(12):2113-2121.
- 10. Australian Institute of Health and Welfare (AIHW). Cancer in Aboriginal and Torres Strait Islander people of Australia. Cancer Series No. 134. Canberra: AIHW; 2023.
- 11. Pimentel-Nunes P, Libânio D, Marcos-Pinto R, et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019. Endoscopy. 2019;51(4):365-388.
- 12. Fitzgerald RC, Hardwick R, Huntsman D, et al. Hereditary diffuse gastric cancer: updated consensus guidelines for clinical management and directions for future research. J Med Genet. 2010;47(7):436-444.
- 13. Wilke H, Muro K, Van Cutsem E, et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): a double-blind, randomised phase 3 trial. Lancet Oncol. 2014;15(11):1224-1235.
- 14. Royal Australasian College of Surgeons (RACS). Upper gastrointestinal cancer surgical outcomes in Australia and New Zealand: National audit report. Melbourne: RACS; 2023.
- 15. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd edition. Sydney: ACSQHC; 2021.