📋 Key Information Summary
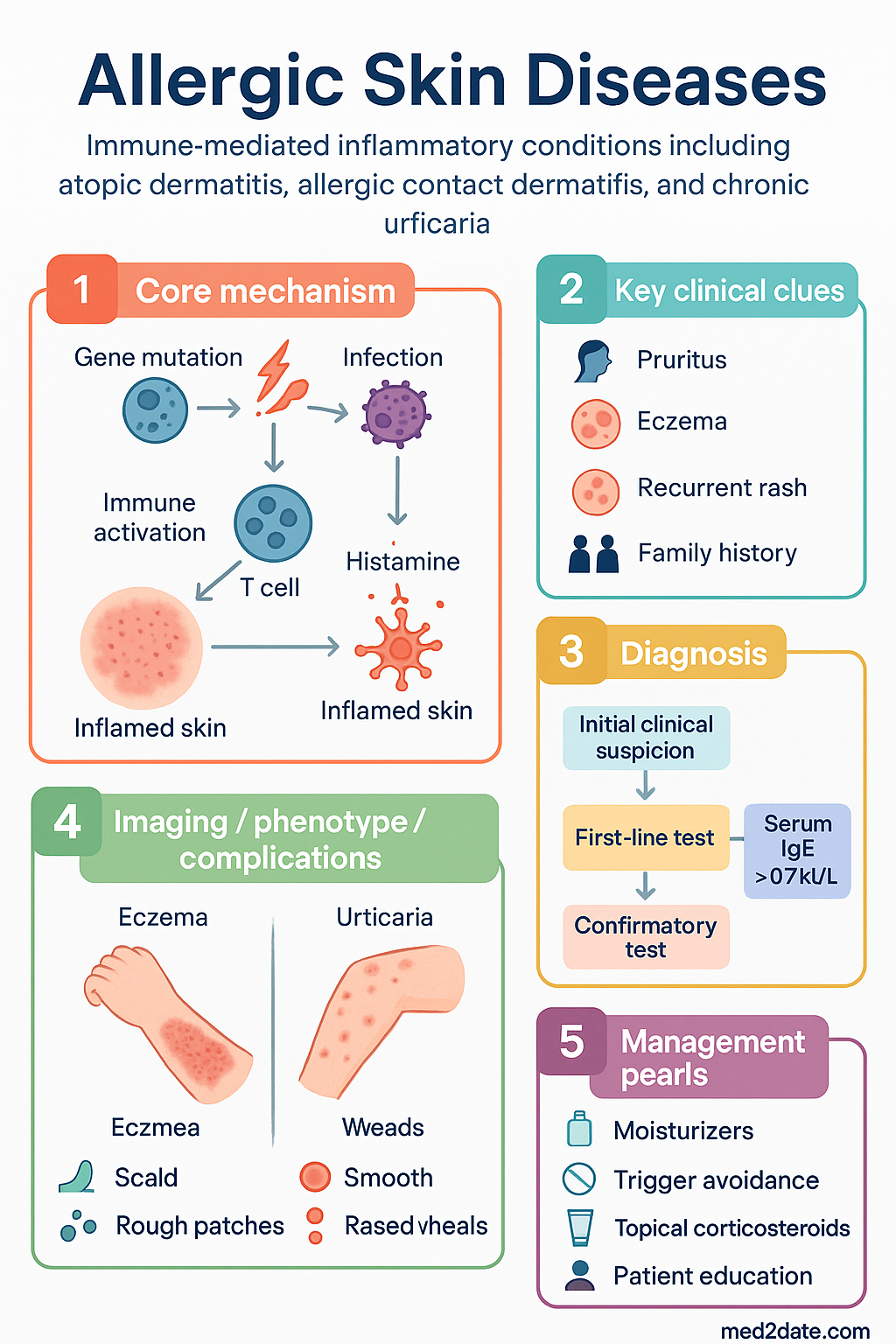
- Allergic skin diseases are immune-mediated inflammatory conditions; the three major types are atopic dermatitis (AD), allergic contact dermatitis (ACD), and chronic urticaria.
- Diagnosis is primarily clinical, guided by history, morphology, and distribution of lesions. Patch testing is the gold standard for ACD.
- Management follows a stepwise approach based on disease severity and chronicity.
- Foundation therapy for all conditions includes patient education, trigger avoidance, and consistent use of emollients.
- First-line pharmacotherapy for mild-moderate AD and ACD is topical corticosteroids (TCS), chosen by potency to suit site and age.
- Topical calcineurin inhibitors (TCIs) are first-line steroid-sparing agents for sensitive skin areas and maintenance therapy.
- For moderate-severe AD, systemic therapy may be required; dupilumab (biologic) is PBS-listed for eligible patients.
- First-line for chronic spontaneous urticaria is a second-generation oral antihistamine, which may be up-dosed.
- Omalizumab is a PBS Authority option for refractory chronic spontaneous urticaria.
- Aboriginal and Torres Strait Islander peoples experience higher prevalence and severity of AD, influenced by environmental and access factors.
- Patient education on correct application of topical therapies (fingertip units) and action plans is critical for adherence and outcomes.
- Consider specialist referral for diagnostic uncertainty, failure of first-line therapy, or need for systemic immunosuppression.
Introduction & Australian Epidemiology
Allergic skin diseases represent a common and heterogeneous group of inflammatory dermatoses driven by dysregulated immune responses to environmental antigens or endogenous factors. They constitute a significant burden on Australian healthcare and quality of life. The major categories include atopic dermatitis (eczema), allergic contact dermatitis, and urticaria.
In Australia, atopic dermatitis is the most prevalent chronic inflammatory skin disease, affecting approximately 10-15% of children and 5-8% of adults. Prevalence has increased over recent decades. Allergic contact dermatitis accounts for up to 20% of occupational dermatitis cases. Chronic urticaria, defined by recurrent wheals for >6 weeks, affects 0.5-5% of the population at any time. These conditions often coexist with other atopic diseases like asthma and allergic rhinitis.
Types & Classification
| Condition | Key Features | Common Triggers |
|---|---|---|
| Atopic Dermatitis (AD) | Chronic, relapsing, pruritic. Flexural distribution in adults; face/extensor in infants. Personal/family history of atopy. | Irritants (soaps, wool), aeroallergens (dust mite), foods (in some children), stress, skin infection. |
| Allergic Contact Dermatitis (ACD) | T-cell mediated, type IV hypersensitivity reaction. Localised to contact site but may become generalised. | Nickel (jewellery), fragrances, preservatives (MCI/MI), rubber accelerators, hair dyes (PPD). |
| Chronic Urticaria | Recurrent, transient wheals ± angioedema lasting >6 weeks. Spontaneous or inducible (dermatographism). | Often idiopathic (autoimmune in ~50%). Physical stimuli (pressure, cold), NSAIDs, pseudoallergens. |
Pathophysiology
Atopic Dermatitis
Involves a complex interplay between skin barrier dysfunction and immune dysregulation. Loss-of-function mutations in the filaggrin gene impair epidermal barrier integrity, leading to increased transepidermal water loss and allergen penetration. This triggers a T-helper 2 (Th2)-predominant immune response, with elevated IgE and cytokines like IL-4, IL-13, and IL-31 (the "itch cytokine").
Allergic Contact Dermatitis
A classic delayed-type hypersensitivity reaction. A low-molecular-weight hapten penetrates the skin and binds to endogenous proteins, forming a complete antigen. This is processed by Langerhans cells, leading to sensitisation and clonal expansion of hapten-specific T-cells. Re-exposure triggers a cell-mediated inflammatory response (eczematous dermatitis).
Chronic Spontaneous Urticaria
Primary effector is the mast cell. In ~50% of cases, it is autoimmune, involving IgG autoantibodies against the high-affinity IgE receptor (FcεRI) or IgE itself, leading to mast cell degranulation. Released histamine and other mediators cause vasodilatation, plasma extravasation (wheal), and sensory nerve activation (pruritus).
Clinical Features
Atopic Dermatitis
- Infants: Cheeks, scalp, extensor surfaces. Oozing, crusted plaques.
- Children/Adults: Flexural folds (antecubital, popliteal fossae). Lichenified, dry, excoriated plaques.
- Signs: Dennie-Morgan infraorbital folds, keratosis pilaris, white dermographism.
Allergic Contact Dermatitis
- Acute: Well-demarcated, erythematous, vesicular, weeping plaques.
- Chronic: Dry, fissured, lichenified plaques.
- Distribution often provides a clue to the allergen (e.g., earlobes from nickel, feet from shoe chemicals).
Chronic Urticaria
- Wheals: Transient, migratory, pruritic, central swelling with surrounding erythema. Individual lesions resolve in <24 hours.
- Angioedema: Deeper, non-pitting swelling of dermis/subcutis (lips, eyelids). May be painful rather than itchy.
Management
Management is multimodal and stepwise, progressing from non-pharmacological measures and topical therapy to systemic agents.
General Measures (All Conditions)
- Patient Education: Nature of disease, chronicity, trigger avoidance.
- Skin Care: Use soap-free washes. Apply emollients liberally and frequently (at least twice daily), even in remission.
- Wet Wraps: For moderate-severe AD flares, using dilute TCS under damp bandages.
Pharmacotherapy by Condition
Atopic Dermatitis
Chronic Spontaneous Urticaria
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples, particularly children, experience a higher prevalence and greater severity of atopic dermatitis compared to non-Indigenous Australians. The burden is amplified by socioeconomic factors, environmental living conditions (e.g., overcrowding, water insecurity), and barriers to accessing healthcare and affordable treatments.
📚 References
- 1. Australasian Society of Clinical Immunology and Allergy (ASCIA). Eczema (Atopic Dermatitis) - for health professionals. 2023. https://www.allergy.org.au
- 2. Australian Institute of Health and Welfare (AIHW). Atopic dermatitis (eczema). Cat. no. PHE 255. Canberra: AIHW; 2021.
- 3. Zuberbier T, et al. The international EAACI/GA²LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy. 2022;77(3):734-766.
- 4. National Health and Medical Research Council (NHMRC). Atopic dermatitis clinical practice guideline. (Endorsed 2022).
- 5. The Royal Australian College of General Practitioners (RACGP). Diagnosis and management of atopic dermatitis in children and adults. Australian Family Physician. 2014;43(10):690-697.
- 6. Department of Health, Australian Government. Pharmaceutical Benefits Scheme (PBS). Schedule online. Accessed 2024.
- 7. Thyssen JP, et al. Contact Allergy in the Era of Globalization: A Narrative Review. Dermatitis. 2023;34(1):7-16.
- 8. Aboriginal and Torres Strait Islander Health Performance Framework. Health System Performance - Access to health services. 2023. https://www.pc.gov.au/ongoing/report-on-government-services/2023/health
- 9. Wollenberg A, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children. J Eur Acad Dermatol Venereol. 2018;32(5):657-682.
- 10. Australian Commission on Safety and Quality in Health Care (ACSQHC). Australian Atlas of Healthcare Variation. 2023. Skin conditions chapter.