📋 Key Information Summary
- Pancreatic cancer — predominantly pancreatic ductal adenocarcinoma (PDAC) — has one of the worst prognoses of any solid malignancy, with an overall 5-year survival rate of approximately 10–13% in Australia.
- In Australia, approximately 4400 new cases are diagnosed annually; incidence is rising by ~1% per year. PDAC is the third leading cause of cancer-related death nationally.
- Key modifiable risk factors include smoking (2–3× risk), chronic pancreatitis, type 2 diabetes mellitus (especially new-onset), obesity, and heavy alcohol use.
- Non-modifiable risk factors include age >60 years, male sex, family history (≥2 first-degree relatives), and hereditary syndromes (Peutz–Jeghers, BRCA1/2, Lynch syndrome, FAMMM).
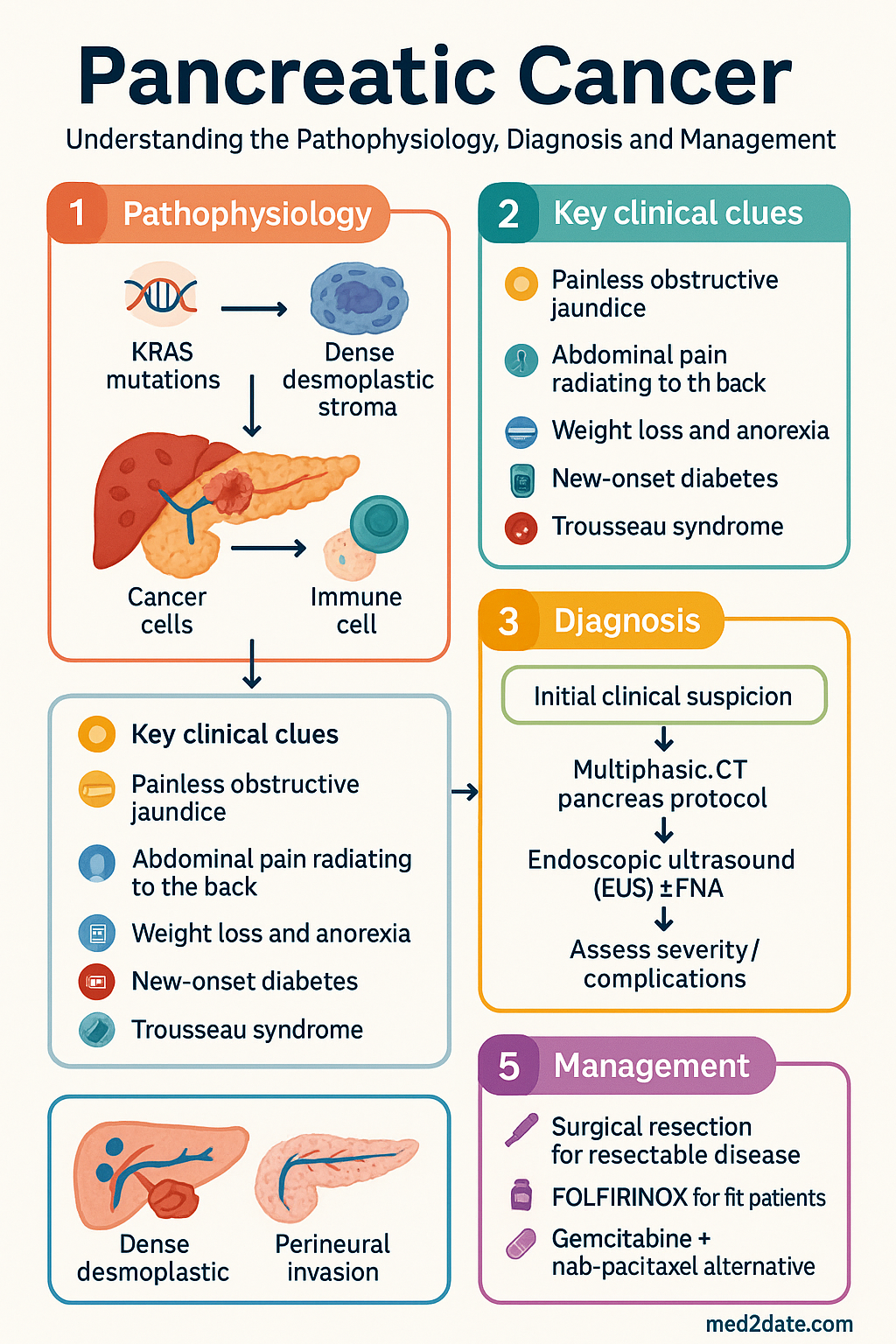
- At diagnosis, only 15–20% of patients are candidates for surgical resection (borderline resectable or resectable disease), which remains the only curative option.
- Whipple procedure (pancreaticoduodenectomy) for head/uncinate tumours; distal pancreatectomy ± splenectomy for body/tail lesions. Operative mortality at high-volume centres is <5%.
- FOLFIRINOX (oxaliplatin, irinotecan, 5-FU, leucovorin) is the preferred first-line regimen for fit patients with good performance status (locally advanced, metastatic, or adjuvant).
- Gemcitabine + nab-paclitaxel is an alternative first-line option, particularly for patients with ECOG 1–2 or significant comorbidity.
- Adjuvant therapy with modified FOLFIRINOX is standard of care after R0/R1 resection for fit patients; 6 months of treatment.
- CA 19-9 is the most useful serum tumour marker for monitoring response, but is unreliable for screening and can be falsely normal in Lewis antigen-negative individuals (~5–10% of population).
- Multidisciplinary team (MDT) review at a high-volume pancreatic centre is mandatory for all cases to optimise staging accuracy and treatment planning.
- Aboriginal and Torres Strait Islander peoples have higher incidence and later-stage presentation; culturally safe, timely access to specialist services and imaging is critical.
- Pancreatic enzyme replacement therapy (PERT) is essential for patients with exocrine insufficiency to optimise nutrition and quality of life.
- Early integration of palliative care improves symptom burden and may extend survival in advanced disease.
Introduction & Australian Epidemiology
Pancreatic cancer predominantly presents as pancreatic ductal adenocarcinoma (PDAC) and carries a very poor prognosis due to late diagnosis, limited surgical resectability, and inherent chemoresistance. It is among the most lethal of all solid organ malignancies, with an overall 5-year survival rate of approximately 10–13% in Australia — a figure that has improved only modestly over the past two decades.
In Australia, pancreatic cancer accounts for approximately 4,400 new diagnoses per year, making it the twelfth most common cancer but the third leading cause of cancer death (after lung and colorectal cancers). Age-standardised incidence has been rising by approximately 1% per year. The median age at diagnosis is 72 years, and males are affected slightly more frequently than females (ratio ~1.2:1).
The disease is characterised by an aggressive biological course, with early perineural and vascular invasion, early metastasis, and a dense desmoplastic stroma that impedes drug delivery. Most patients (80–85%) present with locally advanced or metastatic disease that precludes curative surgical resection.
| Epidemiological Feature | Detail |
|---|---|
| Annual new cases (Australia) | ~4,400 (2024 AIHW estimate) |
| Age-standardised incidence | ~13 per 100,000 per year |
| Median age at diagnosis | 72 years |
| 5-year overall survival | 10–13% |
| Surgically resectable at diagnosis | 15–20% |
| Deaths per year (Australia) | ~3,500 |
Epidemiology & Risk Factors
Modifiable Risk Factors
- Cigarette smoking: The most well-established modifiable risk factor, conferring a 2–3-fold increased risk. Risk declines after cessation but persists for up to 10–15 years. Responsible for approximately 20–25% of all pancreatic cancers.
- Chronic pancreatitis: Confers a 2–6-fold increased risk, with risk rising with duration. Both hereditary and alcohol-related chronic pancreatitis are associated.
- Type 2 diabetes mellitus: Long-standing T2DM increases risk by 1.5–2-fold. New-onset diabetes (<3 years) in patients over 50 may be a presenting feature or early consequence of pancreatic cancer.
- Obesity: BMI >30 kg/m² is associated with a 20–50% increased risk, likely mediated by chronic inflammation and insulin resistance.
- Heavy alcohol consumption: Dose-dependent risk, particularly in the context of chronic pancreatitis.
- Dietary factors: High intake of processed and red meat, low fruit and vegetable consumption — evidence is moderate.
Non-Modifiable & Hereditary Risk Factors
| Risk Factor / Syndrome | Gene(s) | Lifetime Risk | Surveillance Consideration |
|---|---|---|---|
| Peutz–Jeghers syndrome | STK11 | 30–50% | EUS/MRI from age 30 |
| Familial atypical multiple mole melanoma (FAMMM) | CDKN2A | 15–20% | EUS/MRI from age 40 |
| BRCA1/2 mutations | BRCA1, BRCA2 | 3–5% | Consider if family history |
| Hereditary pancreatitis | PRSS1, SPINK1 | 40–50% | EUS/MRI from age 40 |
| Lynch syndrome | MLH1, MSH2, MSH6, PMS2 | 2–4% | As per Lynch surveillance |
| Familial pancreatic cancer (≥2 FDRs) | Multiple | 6–8× | EUS/MRI from age 50 or 10 years before index case |
Pathology & Clinical Features
Histological Subtypes
| Subtype | Frequency | Key Features |
|---|---|---|
| Pancreatic ductal adenocarcinoma (PDAC) | 85–90% | Dense desmoplasia, perineural invasion, KRAS mutations in >90% |
| Intraductal papillary mucinous neoplasm (IPMN) with invasive carcinoma | 3–5% | Mucinous cystic precursor; main-duct type higher risk |
| Pancreatic neuroendocrine tumour (pNET) | 3–5% | Better prognosis; functional vs non-functional |
| Acinar cell carcinoma | 1–2% | Lipase hypersecretion syndrome possible |
| Pancreatoblastoma | <1% | Predominantly paediatric; good prognosis if resected |
Clinical Presentation
Pancreatic cancer is frequently asymptomatic in early stages, and symptoms typically appear only when the tumour has reached a size sufficient to cause local effects or metastatic complications. Common presenting features include:
- Painless obstructive jaundice: Classical presentation for head of pancreas tumours — progressive deepening jaundice with dark urine, pale stools, and pruritus.
- Abdominal pain: Epigastric or left upper quadrant, often radiating to the back. Typically insidious, constant, and worsened by eating or recumbency.
- Weight loss and anorexia: Profound, often >10% body weight, driven by tumour cachexia and exocrine insufficiency.
- New-onset diabetes: Up to 1% of new-onset diabetes in patients >50 years is attributable to occult pancreatic cancer.
- Steatorrhoea: Secondary to pancreatic exocrine insufficiency (maldigestion).
- Trousseau syndrome: Migratory superficial thrombophlebitis or deep vein thrombosis — occurs in 5–10% of PDAC patients.
- Courvoisier sign: Palpable, non-tender gallbladder in the setting of jaundice — more suggestive of periampullary malignancy than gallstone obstruction.
- Depression: New-onset depression in elderly patients without prior psychiatric history may precede cancer diagnosis by months.
Investigations & Staging
Initial Investigations
Resectability Classification (NCCN/International Consensus)
TNM Staging (AJCC 8th Edition)
| Stage | T | N | M | Median Survival |
|---|---|---|---|---|
| IA | T1 (<2 cm) | N0 | M0 | >36 months (if resected) |
| IB | T2 (2–4 cm) | N0 | M0 | 20–30 months (if resected) |
| IIA/IIB | T3 (>4 cm) / any T | N0 / N1 | M0 | 12–20 months (if resected) |
| III | T4 (coeliac/SMA >180°) | Any N | M0 | 9–12 months |
| IV | Any T | Any N | M1 | 3–6 months |
Management — Surgery & Chemotherapy
Surgical Management
Surgical resection remains the only potentially curative treatment for pancreatic cancer. All patients should be discussed at a high-volume multidisciplinary team (MDT) meeting at a centre performing ≥20 pancreatic resections per year.
| Procedure | Indication | Key Considerations |
|---|---|---|
| Pancreaticoduodenectomy (Whipple) | Head / uncinate / ampullary tumours | Pancreaticojejunostomy reconstruction. Pylorus-preserving (ppWhipple) vs classic. Operative mortality <5% at high-volume centres. |
| Distal pancreatectomy ± splenectomy | Body / tail tumours | Spleen preservation (Warshaw technique) if no vascular involvement. Laparoscopic approach acceptable at experienced centres. |
| Total pancreatectomy | Diffuse IPMN, multifocal disease | Brittle insulin-dependent diabetes (Type 3c DM). Lifelong PERT mandatory. Significant morbidity. |
Chemotherapy Regimens
Systemic therapy is the cornerstone of treatment for locally advanced and metastatic pancreatic cancer, and is mandatory as adjuvant therapy after resection. Regimen selection depends on performance status, comorbidities, and molecular profile.
Second-Line Therapy
| Prior Regimen | Second-Line Option | Notes |
|---|---|---|
| Gem/nab-pax → progression | FOLFOX (5-FU + oxaliplatin + leucovorin) or liposomal irinotecan + 5-FU + leucovorin (NAPOLI-1) | Liposomal irinotecan: 70 mg/m² IV q14d + 5-FU 2400 mg/m² CIV 46h + LV 400 mg/m² IV. PBS restricted. |
| FOLFIRINOX → progression | Gemcitabine + nab-paclitaxel | If not previously used. Limited benefit expected. |
| Any → MSI-H/dMMR tumour | Pembrolizumab 200 mg IV q21d | ~1–2% of PDAC. Check MSI/MMR on all patients. Tissue-agnostic PBS listing. |
| Any → NTRK fusion | Larotrectinib 100 mg PO BD or Entrectinib 600 mg PO OD | Extremely rare. Tissue-agnostic approval. |
Adjuvant Therapy After Resection
Radiation Therapy
The role of radiation therapy in pancreatic cancer is evolving and remains controversial. Current Australian practice includes:
- Borderline resectable: Neoadjuvant chemoradiotherapy (e.g., capecitabine-based) may improve R0 resection rates.
- Locally advanced: Consolidation chemoradiotherapy after 4–6 months of systemic therapy if no distant progression (LAP07 trial showed limited benefit).
- Positive margins (R1): Adjuvant radiotherapy may be considered at MDT discretion.
- Stereotactic body radiotherapy (SBRT): Emerging role for locally advanced disease; limited availability in Australia.
Supportive & Palliative Care
Early palliative care integration is recommended from the time of diagnosis for all patients with unresectable disease, and should be offered alongside active treatment for resectable cases.
- Pancreatic enzyme replacement therapy (PERT): Essential for patients with exocrine insufficiency. Pancreatin (Creon®) 25,000–75,000 units lipase with meals and snacks, titrated to symptoms. PBS listed.
- Pain management: WHO analgesic ladder. Coeliac plexus neurolysis (EUS-guided) for refractory pain — superior analgesia and reduced opioid requirement.
- Nutritional support: Early dietitian involvement. Oral nutritional supplements. Consider nasojejunal feeding or PEG only in selected surgical patients.
- Thromboprophylaxis: LMWH (e.g., enoxaparin 40 mg SC OD) recommended for ambulatory patients on chemotherapy due to high VTE risk. Low threshold for investigation of new symptoms.
- Psychosocial support: Cancer Council support services, counselling, advance care planning.
Monitoring & Follow-Up
Post-Resection Surveillance
During Chemotherapy
- FBC, LFTs, renal function before each cycle.
- CA 19-9 every 2–3 months (serial trends more informative than single values).
- CT restaging every 8–12 weeks or with clinical suspicion of progression.
- Neurotoxicity assessment (oxaliplatin — dose reduce or discontinue at grade 2 persistent neuropathy).
- Assess ECOG performance status at each cycle; consider dose modification or treatment break if declining.
Special Populations
Aboriginal and Torres Strait Islander Health
📚 References
- 1. Australian Institute of Health and Welfare (AIHW). Cancer data in Australia: pancreatic cancer. Canberra: AIHW; 2024. Available from: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia
- 2. Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364(19):1817–1825. doi:10.1056/NEJMoa1011923
- 3. Conroy T, Hammel P, Hebbar M, et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med. 2018;379(25):2395–2406. doi:10.1056/NEJMoa1809775
- 4. Von Hoff DD, Ervin T, Arena FP, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369(18):1691–1703. doi:10.1056/NEJMoa1304369
- 5. Golan T, Hammel P, Reni M, et al. Maintenance olaparib for germline BRCA-mutated metastatic pancreatic cancer. N Engl J Med. 2019;381(4):317–327. doi:10.1056/NEJMoa1903387
- 6. National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Pancreatic Adenocarcinoma. Version 2.2024. Available from: https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf
- 7. Royal Australasian College of Surgeons (RACS). Guidelines for the management of pancreatic cancer in Australia and New Zealand. Melbourne: RACS; 2021.
- 8. Cancer Council Australia. Pancreatic cancer — clinical practice guidelines for the management of pancreatic cancer. Sydney: Cancer Council Australia; 2021. Available from: https://www.cancer.org.au/clinical-guidelines/pancreatic-cancer
- 9. Neoptolemos JP, Palmer DH, Ghaneh P, et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet. 2017;389(10073):1011–1024. doi:10.1016/S0140-6736(17)30046-8
- 10. Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 10th ed. East Melbourne: RACGP; 2024.
- 11. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2023: summary report. Canberra: AIHW; 2023.
- 12. Tempero MA, Malafa MP, Al-Hawary M, et al. Pancreatic adenocarcinoma, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19(4):439–457.
- 13. Department of Health and Aged Care, Australian Government. Medicare Benefits Schedule (MBS) — Diagnostic imaging items. Canberra; 2024. Available from: http://www.mbsonline.gov.au