📋 Key Information Summary
- Sulfonamide allergy encompasses hypersensitivity reactions to sulfonamide-class medications, most commonly sulfamethoxazole in co-trimoxazole (trimethoprim–sulfamethoxazole).
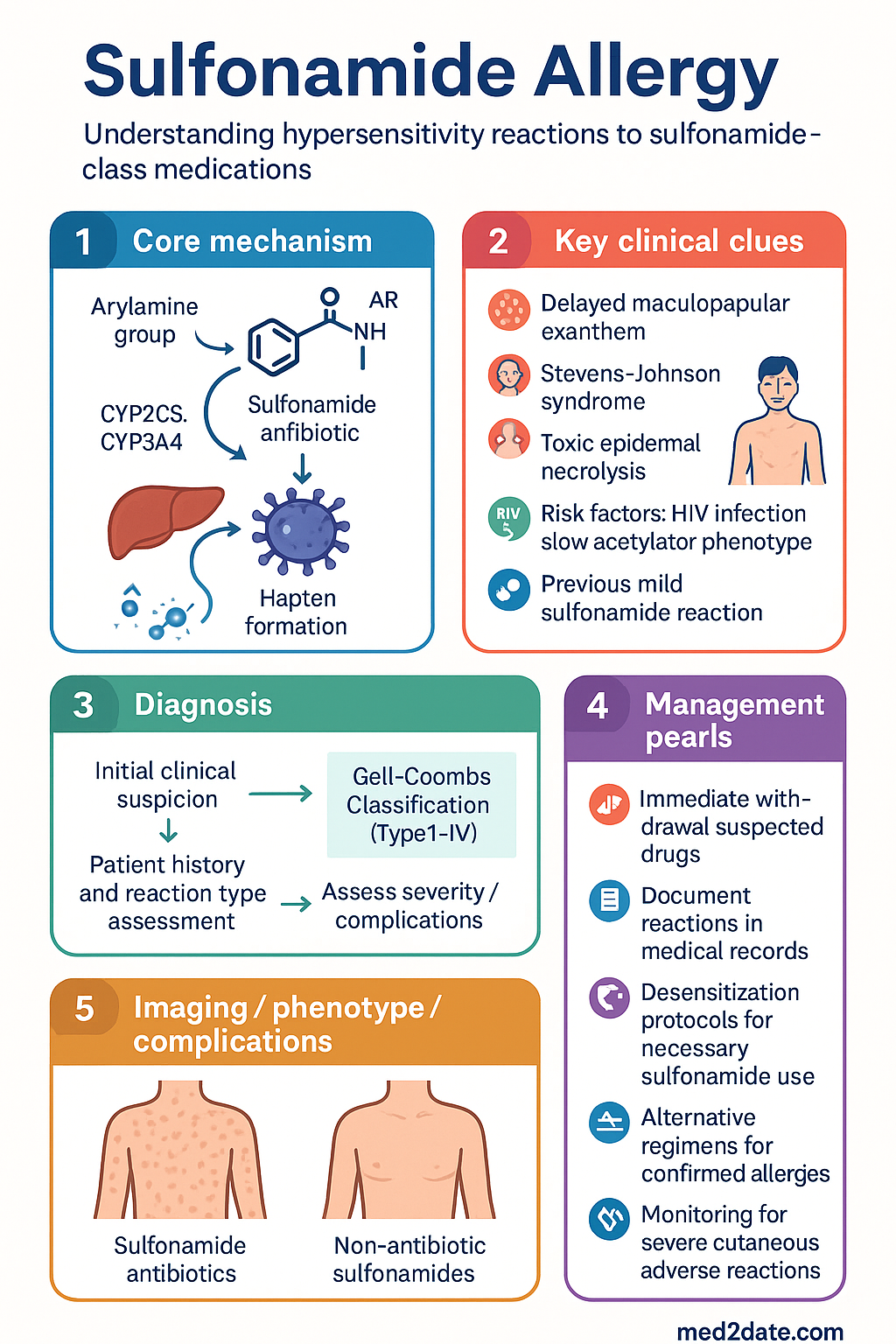
- Reactions range from mild cutaneous eruptions (>90%) to severe, life-threatening conditions including Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN).
- The arylamine hypothesis explains immunological reactions: metabolism of the arylamine group (present in sulfonamide antibiotics but not non-antibiotic sulfonamides) generates reactive hydroxylamine and nitroso metabolites that trigger immune responses.
- Cross-reactivity risk between sulfonamide antibiotics and non-antibiotic sulfonamides (e.g., celecoxib, furosemide, thiazides) is extremely low (<1%) and generally not clinically relevant due to differing chemical structures.
- True IgE-mediated (Type I) reactions to sulfonamides are uncommon; most hypersensitivity reactions are T-cell-mediated (Type IV), typically occurring 7–14 days after initiation.
- Delayed maculopapular exanthem is the most frequent presentation; fixed drug eruptions, urticaria, and serum sickness-like reactions also occur.
- Desensitisation protocols are available for patients requiring co-trimoxazole, particularly for Pneumocystis jirovecii prophylaxis in immunocompromised patients.
- Co-trimoxazole is the first-line agent for several Australian conditions including uncomplicated UTI and Pneumocystis prophylaxis — confirmed allergy necessitates documented alternative regimens.
- Skin prick and intradermal testing for sulfonamides have limited sensitivity and are not routinely recommended in Australian allergy practice.
- All reactions must be clearly documented in the patient's medical record, the Australian Immunisation Register (where applicable), and My Health Record.
- Risk factors for severe reactions include HIV infection, slow acetylator phenotype, concurrent corticosteroid use, and previous mild sulfonamide reaction.
- Remote and regional Australian populations may face limited access to alternative antimicrobials, making careful allergy classification and desensitisation pathways essential.
Introduction & Australian Epidemiology
Sulfonamide allergy refers to hypersensitivity reactions to sulfonamide-containing medications, ranging from mild cutaneous eruptions to severe, life-threatening dermatological and systemic reactions such as Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN). The term most commonly applies to reactions triggered by sulfonamide antibiotics — primarily co-trimoxazole (trimethoprim–sulfamethoxazole) — but historically has been used more broadly to encompass structurally related non-antibiotic sulfonamides.
In Australia, self-reported sulfa allergy prevalence ranges from 3–6% of the general population, making it one of the most commonly documented drug allergies in medical records. Co-trimoxazole is widely prescribed in primary care for urinary tract infections, skin and soft tissue infections, and as prophylaxis against Pneumocystis jirovecii pneumonia (PJP) in immunocompromised individuals. The Australian Commission on Safety and Quality in Health Care (ACSQHC) has identified drug allergy documentation as a key safety priority under the National Safety and Quality Health Service (NSQHS) Standards.
Studies suggest that up to 90% of patients labelled with "sulfonamide allergy" do not have a true immunologically mediated reaction upon formal evaluation, yet the label persists and may result in the use of less effective, broader-spectrum, or more toxic alternatives. Accurate classification of the reaction type is essential to optimise antimicrobial stewardship and patient outcomes across Australian healthcare settings.
Mechanisms of Reaction
Understanding the immunological mechanisms underlying sulfonamide hypersensitivity is essential for accurate diagnosis, risk stratification, and safe therapeutic planning. Sulfonamide reactions involve multiple immunological pathways and non-immunological mechanisms.
The Arylamine Hypothesis
The predominant immunological mechanism for sulfonamide antibiotic reactions involves metabolic activation of the arylamine moiety present in sulfonamide antibiotics (e.g., sulfamethoxazole). Cytochrome P450 enzymes (particularly CYP2C9 and CYP3A4) convert the arylamine group to reactive hydroxylamine and nitroso intermediates. These metabolites act as haptens, covalently binding to endogenous proteins and forming immunogenic neoantigens that activate both humoral and cell-mediated immune responses.
This mechanism explains why sulfonamide antibiotics carry a substantially higher risk of hypersensitivity compared to non-antibiotic sulfonamides (such as furosemide, celecoxib, or thiazide diuretics), which lack the arylamine group and undergo different metabolic pathways.
Gell–Coombs Classification of Sulfonamide Reactions
| Type | Mechanism | Timing | Clinical Features |
|---|---|---|---|
| Type I (Immediate) | IgE-mediated mast cell degranulation | Minutes to hours | Urticaria, angioedema, anaphylaxis (rare with sulfonamides) |
| Type II (Cytotoxic) | IgG/IgM-mediated cytotoxicity | Hours to days | Haemolytic anaemia, thrombocytopenia, agranulocytosis |
| Type III (Immune complex) | Immune complex deposition | 7–21 days | Serum sickness-like reaction, drug-induced vasculitis |
| Type IV (Delayed) | T-cell-mediated (most common) | 7–14 days (up to 21 days) | Maculopapular exanthem, DRESS, SJS, TEN, fixed drug eruption |
Type IV Subtypes in Sulfonamide Hypersensitivity
- Type IVa (Th1-mediated): Maculopapular exanthema; IFN-γ-driven inflammation
- Type IVb (Th2-mediated): Drug reaction with eosinophilia and systemic symptoms (DRESS); IL-4, IL-5, IL-13 involvement
- Type IVc (Cytotoxic T-cell): SJS and TEN; perforin/granzyme B-mediated keratinocyte apoptosis
- Type IVd (Neutrophilic): Acute generalised exanthematous pustulosis (AGEP); IL-8/CXCL8-mediated neutrophil recruitment
Non-Immunological Mechanisms
Some adverse effects of sulfonamides are not mediated by immune mechanisms:
- Dose-related toxicity: Hyperkalaemia (from trimethoprim inhibition of ENaC channels), crystalluria, kernicterus in neonates
- Competitive antagonism: Sulfonamides competitively inhibit folate synthesis in susceptible organisms; in humans, this may cause megaloblastic anaemia with prolonged high-dose use
- Pharmacogenomic predisposition: Slow N-acetyltransferase 2 (NAT2) acetylator phenotype results in accumulation of reactive metabolites, increasing risk of hypersensitivity
Genetic Risk Factors
HLA associations with sulfonamide hypersensitivity have been identified in various populations. HLA-B*38:02 has been associated with co-trimoxazole-induced SCARs in European populations. Pharmacogenomic testing is not yet standard of care in Australia but may become relevant for high-risk populations as precision medicine advances.
Clinical Presentations
Sulfonamide hypersensitivity manifests across a broad clinical spectrum. Accurate characterisation of the presenting reaction is critical for determining safety of future sulfonamide exposure and guiding allergy documentation.
Detailed Clinical Manifestations
Mild Reactions
- Delayed maculopapular exanthem: Onset typically 7–14 days after commencing therapy; morbilliform, symmetric, pruritic eruption often beginning on the trunk. May be accompanied by low-grade fever. Resolves within 7–14 days of drug cessation.
- Fixed drug eruption: Well-demarcated, round, erythematous to violaceous plaques recurring at the same anatomical site upon re-exposure. Mucosal surfaces may be affected. Occurs within 30 minutes to 8 hours of re-exposure.
- Isolated urticaria: True IgE-mediated urticaria to sulfonamides is uncommon. Most urticarial presentations represent a manifestation of a Type IV reaction.
Moderate Reactions
- Drug reaction with eosinophilia and systemic symptoms (DRESS): Characterised by the triad of extensive cutaneous eruption, haematological abnormalities (eosinophilia, atypical lymphocytosis), and internal organ involvement (hepatitis, nephritis, pneumonitis, myocarditis). Onset 2–6 weeks after initiation; may flare for weeks after drug cessation. Mortality 5–10%, primarily from hepatic necrosis.
- Serum sickness-like reaction: Fever, arthralgia, urticaria, and lymphadenopathy occurring 7–21 days after exposure. Unlike true serum sickness, immune complex deposition is typically absent.
- Acute generalised exanthematous pustulosis (AGEP): Acute onset of widespread sterile pustules on erythematous background, fever, neutrophilia. Usually resolves within 2 weeks of drug withdrawal.
Severe Reactions — Requiring Emergency Management
- Prodrome of fever, malaise, stinging eyes, painful swallowing 1–3 days before rash onset
- Dusky erythematous macules and targetoid lesions progressing to epidermal detachment
- Nikolsky sign positive (lateral pressure causes epidermal sliding)
- Haemorrhagic crusting of lips; conjunctival injection, pseudomembrane formation
- Immediate withdrawal of all suspected drugs, referral to burns unit/ICU
Organ-Specific Non-Cutaneous Reactions
- Haematological: Haemolytic anaemia (Coombs-positive), thrombocytopenia, agranulocytosis, methaemoglobinaemia
- Hepatic: Cholestatic or hepatocellular hepatitis, particularly in DRESS
- Renal: Acute interstitial nephritis, crystalluria with inadequate hydration
- Pulmonary: Eosinophilic pneumonia, pulmonary infiltrates
- Neurological: Aseptic meningitis (rare, particularly with trimethoprim component)
Cross-Reactivity
Cross-reactivity between sulfonamide antibiotics and other sulfonamide-containing or sulfite-containing medications is a common clinical concern, yet the evidence overwhelmingly indicates that true cross-reactivity is exceedingly rare.
Sulfonamide Antibiotics vs Non-Antibiotic Sulfonamides
| Feature | Antibiotic Sulfonamides | Non-Antibiotic Sulfonamides |
|---|---|---|
| Examples | Sulfamethoxazole, sulfadiazine, sulfadoxine, sulfasalazine | Celecoxib, furosemide, thiazide diuretics, sumatriptan, topiramate, dorzolamide, probenecid |
| Arylamine group | Present — primary determinant of immunogenicity | Absent |
| Reactive metabolite formation | Yes (hydroxylamine, nitroso via CYP2C9/3A4) | No |
| Cross-reactivity risk | Between sulfonamide antibiotics: moderate (3–40% in some studies) | Extremely low (<1%); not clinically significant |
Cross-Reactivity Among Sulfonamide Antibiotics
Cross-reactivity between different sulfonamide antibiotics (e.g., sulfamethoxazole and sulfadiazine) is more plausible, as they share the arylamine group and similar metabolic pathways. Studies suggest cross-reactivity rates of 3–40%, though methodological limitations make precise estimates difficult.
Sulfites — A Common Misconception
Sulfites (sodium metabisulfite, sulfur dioxide) used as preservatives in foods and medications are not structurally related to sulfonamides. Patients with sulfonamide allergy do not have an increased risk of sulfite sensitivity. Sulfite reactions are typically respiratory (bronchospasm in asthmatics) and are mediated by a completely different mechanism.
Clinical Recommendations for Cross-Reactivity Assessment
Management & Alternatives
Management of sulfonamide allergy involves acute treatment of the reaction, accurate allergy documentation, selection of appropriate therapeutic alternatives, and consideration of desensitisation when sulfonamide therapy is clinically necessary.
Acute Management of Sulfonamide Hypersensitivity
Therapeutic Alternatives by Clinical Indication
Urinary Tract Infection (Uncomplicated)
Pneumocystis jirovecii Pneumonia Prophylaxis
Co-trimoxazole is the gold-standard PJP prophylactic agent. When true sulfonamide allergy exists, the following alternatives are used:
Toxoplasmosis Prophylaxis
Co-trimoxazole also provides concurrent Toxoplasma gondii prophylaxis. If sulfonamide allergy precludes co-trimoxazole, add pyrimethamine + leucovorin to the alternative PJP prophylaxis regimen:
- Pyrimethamine: 25–50 mg PO weekly + leucovorin 25 mg PO weekly (to prevent myelosuppression)
- Monitor FBC fortnightly for first month, then monthly
Desensitisation Protocols
Drug desensitisation may be considered when sulfonamide therapy is essential and no suitable alternative exists. This procedure should only be undertaken in a supervised hospital setting with resuscitation capabilities.
Rapid Oral Desensitisation Protocol (Modified Trimethoprim–Sulfamethoxazole)
The following is a commonly used 12-step protocol adapted from Australian and international immunology references:
| Step | SMX dose (mg) | Cumulative SMX (mg) | Interval |
|---|---|---|---|
| 1 | 0.02 | 0.02 | 15 min |
| 2 | 0.04 | 0.06 | 15 min |
| 3 | 0.1 | 0.16 | 15 min |
| 4 | 0.2 | 0.36 | 15 min |
| 5 | 0.4 | 0.76 | 15 min |
| 6 | 1 | 1.76 | 15 min |
| 7 | 2 | 3.76 | 15 min |
| 8 | 5 | 8.76 | 15 min |
| 9 | 10 | 18.76 | 15 min |
| 10 | 25 | 43.76 | 15 min |
| 11 | 50 | 93.76 | 15 min |
| 12 | 160 (full dose) | 253.76 | — |
Each dose is diluted in water or administered as oral suspension. Continuous cardiac monitoring and IV access should be maintained. If a reaction occurs at any step, treat the reaction and consider repeating the same dose or the previous tolerated dose.
Allergy Documentation & Discharge Planning
- Document the specific sulfonamide drug, dose, route, date, and detailed reaction description
- Classify as: mild (non-SCAR) vs severe (SCAR) — this distinction is critical for future management
- Specify which sulfonamide-containing medications are and are not safe (e.g., "Allergy to sulfamethoxazole — may use celecoxib, furosemide safely")
- Update My Health Record Shared Health Summary
- Provide patient with a written allergy card for presentation at all healthcare encounters
- For hospitalised patients: alert pharmacy, nursing, and all treating teams
- Refer to clinical immunology/allergy for formal evaluation if not already completed
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Investigations
Investigation of suspected sulfonamide hypersensitivity combines clinical history, laboratory testing, and in selected cases, specialist allergy testing. There is no single confirmatory test for sulfonamide allergy.
📚 References
- 1. Strom BL, Schinnar R, Apter AJ, et al. Absence of cross-reactivity between sulfonamide antibiotics and sulfonamide nonantibiotics. N Engl J Med. 2003;349(17):1628-1635.
- 2. Brackett CC, Singh H, Block JH. Likelihood and mechanisms of cross-allergenicity between sulfonamide antibiotics and other drugs containing a sulfonamide functional group. Pharmacotherapy. 2004;24(7):856-870.
- 3. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 4. Rieder MJ, Uetrecht J, Shear NH, Cannon M, Miller M, Spielberg SP. Diagnosis of sulfonamide hypersensitivity reactions by in-vitro "rechallenge" with hydroxylamine metabolites. Ann Intern Med. 1989;110(4):286-289.
- 5. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health; 2022. Available at: immunisationhandbook.health.gov.au.
- 6. Australian Indigenous HealthInfoNet. Summary of Aboriginal and Torres Strait Islander health. Perth: Edith Cowan University; 2023.
- 7. Hsu DY, Brieva J, Silverberg NB, Silverberg JI. Morbidity and mortality of Stevens-Johnson syndrome and toxic epidermal necrolysis in United States adults. J Invest Dermatol. 2016;136(7):1387-1397.
- 8. Shiohara T, Inaoka M, Kano Y. Drug-induced hypersensitivity syndrome (DIHS): a reaction induced by a complex interplay among herpesviruses and antiviral and antidrug immune responses. Allergol Int. 2006;55(1):1-8.
- 9. Sullivan TJ, Ong YC, Gilliam LK. Studies of the multiple drug allergy syndrome. J Allergy Clin Immunol. 1989;83(1):198-207.
- 10. Royal Australian College of General Practitioners (RACGP). Prescribing drugs of dependence in general practice, Part A: Antibiotics. Melbourne: RACGP; 2023.
- 11. Australasian Society of Clinical Immunology and Allergy (ASCIA). Drug allergy — clinical update. Sydney: ASCIA; 2023. Available at: allergy.org.au.
- 12. AIHW (Australian Institute of Health and Welfare). Aboriginal and Torres Strait Islander health performance framework 2023 summary report. Canberra: AIHW; 2023.
- 13. Blumenthal KG, Peter JG, Trubiano JA, Phillips EJ. Antibiotic allergy. Lancet. 2019;393(10167):183-198.
- 14. Trubiano JA, Worth LJ, Urbancic K, et al. Return to sender: the need to re-address patient antibiotic allergy labels in Australia. Intern Med J. 2016;46(11):1311-1317.