Definition: Juvenile nasopharyngeal angiofibroma (JNA) is a benign vascular locally aggressive neoplasm of the nasopharynx.
Age and incidence:
It accounts for 0.5% of all head and neck tumors occurring in 1 of 150,000 individuals.
Adolescents and young adults between 14 and 25 years are affected, and there is a distinct male predominance. JNA may occur in older patients as well. The prevalence in males may be explained by high androgen receptor (AR) expression suggesting that JNA is androgen dependent.
Etiology (causes) of nasopharyngeal angiofibroma:
Causes of JNA are not fully understood:
- Hamartoma and vascular malformation theories.
- JNA's sex selectivity and the relatively young age suggest that it is hormone dependent.
- Chemodectoma from the paraganglionic cells at the terminal end of the maxillary artery.
Pathology:
It is a lobulated firm mass with no true capsule.
Microscopically:
- Vascular Component: Many large sinusoidal spaces with no muscular coat hence they bleed profusely having no contractile element.
- Fibrous Component: Stroma of coarse parallel or interlacing collagen bundles. By time the fibrous component exceeds the vascular component.
Origin and spread:
- It arises adjacent to the sphenopalatine foramen in the posterosuperior wall of the nasal cavity.
- Large tumors are frequently bilobed or dumbbell-shaped, with one portion filling the nasopharynx and the other in the pterygopalatine fossa.
- Anterior growth occurs under the nasopharyngeal mucous membrane, displacing it anteriorly toward the postnasal space. Eventually, the nasal cavity is filled on one side, and the septum deviates to the other side.
- Superior growth is directed toward the sphenoid sinus. The cavernous sinus may become invaded if the tumor advances further.
- Lateral spread is directed toward the pterygopalatine fossa, bowing the posterior wall of the maxillary sinus. Later, the infratemporal fossa is invaded.
- Proptosis and optic nerve atrophy result if the inferior orbital fissures are encroached.
- Rarely spontaneous regression occurs at the age of sexual maturity.
Symptoms of nasopharyngeal angiofibroma:
- Nasal obstruction (80-90%).
- Epistaxis (45-60%) - Mostly unilateral, severe and recurrent.
- Headache (25%) - Especially if paranasal sinuses are blocked.
- Facial swelling (10-18%)
- Other symptoms: Unilateral rhinorrhea, hyposmia, rhinolalia, deafness, otalgia, palatal swelling and deformity of the cheek
Signs:
- Nasal mass (80%), orbital mass (15%), and proptosis (10-15%).
- Other signs include serous otitis due to eustachian tube blockage, zygomatic swelling, and trismus that denote spread of the tumor to the infratemporal fossa, (rare).
Differential Diagnosis of nasopharyngeal angiofibroma:
- Other causes of nasal obstruction, (eg. antrochoanal polyp and inverting papilloma).
- Other causes of epistaxis, systemic or local.
- Other causes of proptosis or orbital swellings.
Investigations to confirm diagnosis:
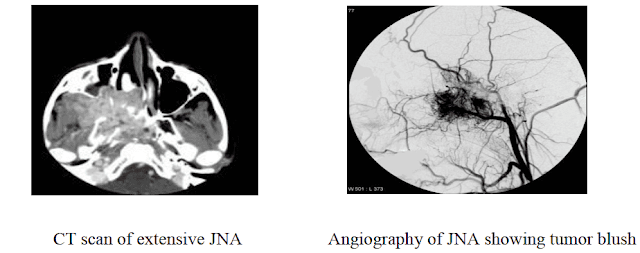
- CT: it is particularly useful at delineating bony changes. Typically a lobulated non-encapsulated soft tissue mass is demonstrated centred on the sphenopalatine foramen (which is often widened) and usually bowing the posterior wall of the maxillary antrum anteriorly. There is marked contrast enhancement reflecting the prominent vascularity.
- Angiography is often useful in defining the feeding vessels as well as in preoperative embolization. Supply of these tumors is usually via internal maxillary artery, ascending pharyngeal artery and palatine artery. Internal carotid artery may supply large tumors.
- MR and MR angiography are excellent at evaluating tumor extension especially into the orbit and intracranial compartments.
- Biopsy is contraindicated due to the risk of severe epistaxis, Diagnosis of JNA is based on clinical and radiological evaluation.
Treatment of nasopharyngeal angiofibroma:
Surgical treatment: surgical excision is the treatment of choice. The surgical approach depends on the size and extent of JNA. Examples are transpalatal, lateral rhinotomy, transnasal-tranantral and degloving approach.
However, now most cases can be removed endoscopically.
Preoperative embolization of the feeding vessels is done 2-3 days before surgery to minimize bleeding.
In cases of large and extensive vascular tumor preoperative tracheostomy may be considered for fear of blood aspiration and stridor due to postoperative edema.
Radiotherapy: Not used due to its carcinogenic effect, except in some cases with inoperable intracranial extension..
Hormonal Therapy: (controversial)