📋 Key Information Summary
- Hepatocellular carcinoma (HCC) is the most common primary liver cancer, accounting for ~85% of cases, and typically arises in the setting of chronic liver disease and cirrhosis.
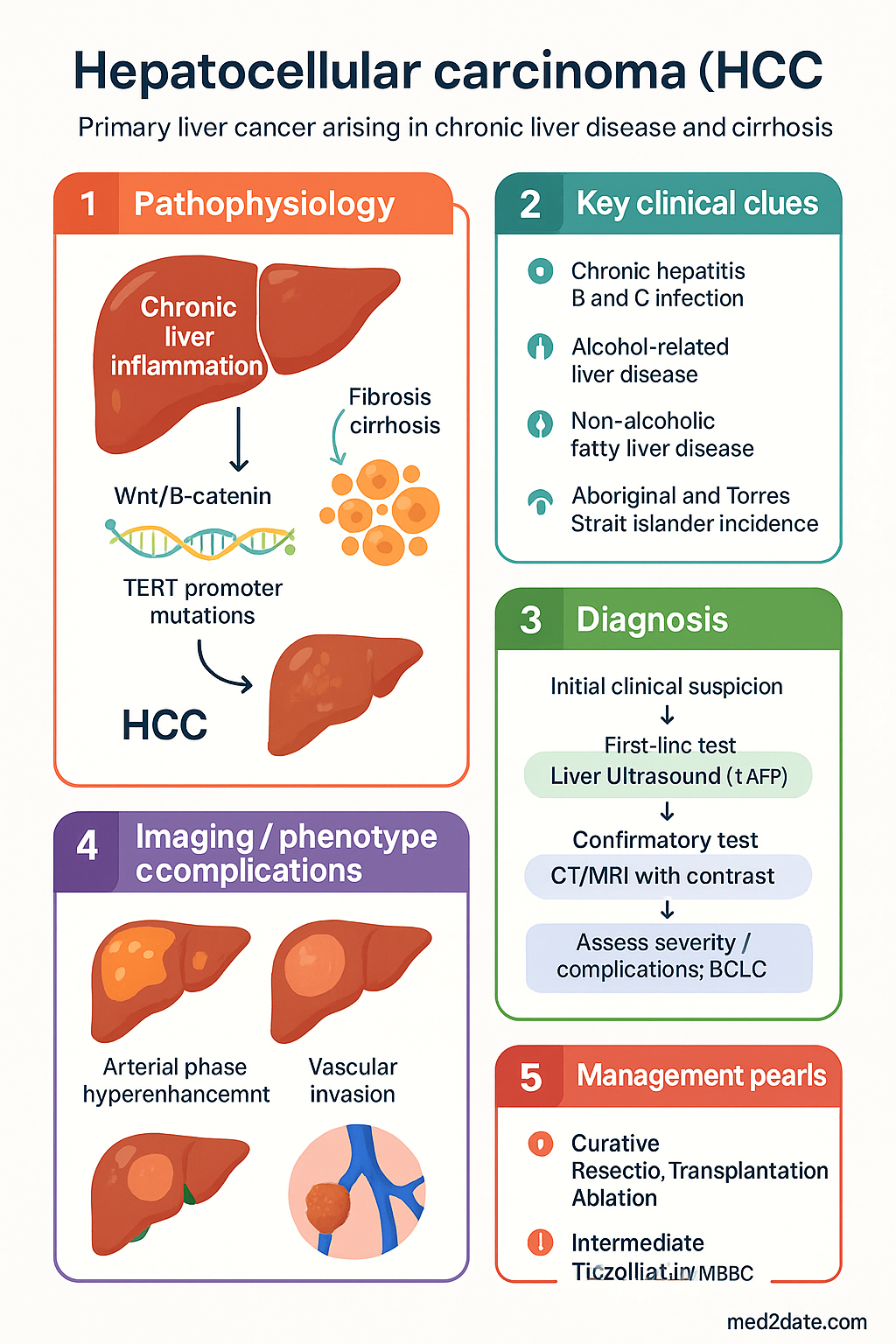
- Key risk factors in Australia include chronic hepatitis B (HBV) and C (HCV) infection, alcohol-related liver disease, and non-alcoholic fatty liver disease (NAFLD).
- Aboriginal and Torres Strait Islander peoples experience higher incidence and poorer outcomes due to disparities in risk factor prevalence and healthcare access.
- Surveillance with six-monthly liver ultrasound (± alpha-fetoprotein) is recommended for at-risk groups to enable early detection when curative treatment is possible.
- Diagnosis is primarily imaging-based (CT/MRI with contrast) using LI-RADS criteria; biopsy is reserved for indeterminate cases.
- Staging and treatment allocation follow the Barcelona Clinic Liver Cancer (BCLC) system, which integrates tumour burden, liver function (Child-Pugh), and performance status.
- Potentially curative treatments for very early/early stage (BCLC 0/A) include surgical resection, liver transplantation, and local ablation (e.g., radiofrequency ablation).
- For intermediate stage (BCLC B), transarterial chemoembolisation (TACE) is the standard of care.
- Systemic therapy is indicated for advanced BCLC C disease. First-line options include atezolizumab + bevacizumab or sorafenib.
- Sorafenib (Nexavar®) is a PBS Authority Required multi-kinase inhibitor that modestly improves overall survival. It requires careful management of side effects like hand-foot skin reaction and hypertension.
- Multidisciplinary team (MDT) discussion is mandatory for all patients to tailor management based on tumour stage, liver function, and comorbidities.
- Management of underlying cirrhosis and its complications (e.g., portal hypertension, varices) is integral to HCC care.
Introduction & Australian Epidemiology
Hepatocellular carcinoma (HCC) is a major global health burden and the most common primary malignancy of the liver. In Australia, it is one of the few cancers with increasing incidence and mortality rates. The disease typically arises in the context of chronic liver inflammation and fibrosis/cirrhosis, which provides a premalignant field. The landscape of HCC management is complex, requiring integration of tumour staging, assessment of underlying liver function, patient fitness, and available curative or palliative modalities. This guideline provides a framework for the investigation and management of HCC within the Australian healthcare context.
In Australia, the age-standardised incidence rate of liver cancer (predominantly HCC) has more than tripled over the past three decades. According to the Australian Institute of Health and Welfare (AIHW), it was the sixth most common cause of cancer death in 2022. Chronic viral hepatitis, particularly hepatitis B (HBV) and hepatitis C (HCV), remains the leading attributable risk factor. However, the incidence of HCC associated with non-alcoholic fatty liver disease (NAFLD) and alcohol-related liver disease (ALD) is rising sharply. There is a significant disparity in burden, with Aboriginal and Torres Strait Islander peoples experiencing approximately twice the incidence and poorer survival outcomes compared to non-Indigenous Australians.
Epidemiology & Risk Factors
The development of HCC is a multi-step process strongly associated with the presence of cirrhosis, regardless of aetiology. Understanding the major risk factors is crucial for targeting surveillance programmes.
| Risk Factor | Estimated Population Attributable Risk (Australia) | Key Points |
|---|---|---|
| Chronic Hepatitis B (HBV) | ~25-30% | Major risk even without cirrhosis. Higher prevalence in those born in endemic regions and Aboriginal and Torres Strait Islander communities. Vaccination is preventative. |
| Chronic Hepatitis C (HCV) | ~20-25% | Risk persists after cirrhosis has developed, even if SVR is achieved with direct-acting antivirals (DAAs). Surveillance continues post-cure if cirrhosis is present. |
| Alcohol-related Liver Disease (ALD) | ~20-25% | Risk is dose- and duration-dependent, primarily in those with established cirrhosis. |
| Non-Alcoholic Fatty Liver Disease (NAFLD) | ~15-20% (and rising) | The fastest-growing risk factor. HCC can occur in NAFLD without cirrhosis, particularly in the context of metabolic syndrome. |
| Other | ~5-10% | Includes haemochromatosis, autoimmune hepatitis, alpha-1 antitrypsin deficiency, and Wilson disease. |
Pathogenesis & Barcelona Clinic Liver Cancer (BCLC) Staging
Hepatocarcinogenesis is driven by chronic necro-inflammation, regenerative nodularity, and accumulation of genetic and epigenetic alterations. The cirrhotic microenvironment with altered growth signalling (e.g., Wnt/β-catenin, TERT promoter mutations) facilitates malignant transformation.
Staging in HCC serves a dual purpose: prognostication and treatment allocation. The Barcelona Clinic Liver Cancer (BCLC) system is the internationally endorsed and widely used standard in Australia. It classifies patients into five stages linked to specific treatment strategies.
Investigations & Surveillance
Surveillance Program
Aim to detect HCC at a curable stage. The primary modality is six-monthly abdominal ultrasound. The role of alpha-fetoprotein (AFP) as an adjunct is debated but often used in conjunction.
Diagnostic Workup
Diagnosis of HCC in cirrhotic liver can often be made non-invasively using contrast-enhanced imaging (LI-RADS 5: arterial phase hyperenhancement + washout/capsule).
Staging Workup
Treatment (Resection, Ablation & Sorafenib)
Treatment is highly stage-dependent. All patients must be discussed in a specialist Multidisciplinary Team (MDT) meeting including hepatobiliary surgery, transplant surgery, hepatology, medical oncology, interventional radiology, and radiation oncology.
Curative-Intent Treatments (BCLC 0/A)
Systemic Therapy for Advanced HCC (BCLC C)
First-line systemic therapy has evolved significantly. The combination of atezolizumab (PD-L1 inhibitor) and bevacizumab (anti-VEGF) has become the preferred regimen based on superior overall survival data. Sorafenib remains a key standard-of-care option, particularly where immunotherapy is contraindicated.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Cancer Council Australia. Liver Cancer – Guidelines for Health Professionals. Sydney: Cancer Council Australia; 2023.
- 2. Australian Institute of Health and Welfare (AIHW). Cancer data in Australia 2022. Cat. no. CAN 141. Canberra: AIHW; 2023.
- 3. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J Hepatol. 2022;76(3):681-693.
- 4. The Royal Australian College of General Practitioners (RACGP). Hepatitis B and C: Management in Primary Care. 2nd ed. East Melbourne: RACGP; 2022.
- 5. Pharmaceutical Benefits Scheme (PBS). Sorafenib (Nexavar®) Authority Required PBS item. Australian Government Department of Health. Accessed October 2023.
- 6. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N Engl J Med. 2020;382(20):1894-1905.
- 7. Transplantation Society of Australia and New Zealand (TSANZ). Liver Transplantation Guidelines. 2021.
- 8. National Health and Medical Research Council (NHMRC). Strengthening the diagnosis and management of chronic hepatitis B in Aboriginal and Torres Strait Islander peoples. 2020.
- 9. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 10. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723-750.