Nasopharyngeal carcinoma (NPC) represents 80% of nasopharyngeal malignant tumors, but in general, it is a rare tumor with an incidence rate of 1% of all childhood malignancies. It arises from the epithelial lining of the nasopharynx (the upper part of the throat, behind the nose).

What is nasopharynx? It is the part of the pharynx that is located at the base of the skull, above the roof of the mouth. Nostrils open into the nasopharynx. When you breathe, air flows through your nose into your throat and nasopharynx, and eventually into your lungs.

Age, sex and distribution of Nasopharyngeal cancer
Nasopharyngeal carcinoma is more common in males than females (ratio 3:1), and it occurs more commonly above the age of 40 years old. Geographically, it is more in China, Sudan, Yemen. Children of Asian, Middle Eastern, and Northern African descent are also more commonly affected
Causes and predisposing factors
- Cigarette Smoking
- Infection by Epstein Barr Virus (EBV) [Though scientists don't its exact cause, but nasopharyngeal cancer is strongly linked to EBV]
- Inhalation of formaldehyde & hydrocarbons
- Human leucocytic antigen (HLA)
N.B: Having EBV infection doesn't mean that you will get nasopharyngeal cancer, it is just a predisposing factor. Scientists think that the DNA of the virus affects and changes the DNA of the cells of the nasopharynx, this change causes cells to grow and divide abnormally.
Pathology:
Site of origin: any part of nasopharynx, but most common from fossa of RosenMuller, a space above and posterior to Eustachian tube orifice (one of silent areas of head and neck).
Side: usually begins unilateral then crosses midline to other side.
Gross picture: Reddish fungating mass or malignant ulcer.
Microscopic picture: squamous cell carcinoma is the commonest.
Histological types of nasopharyngeal carcinoma (WHO classification) are:
- Type 1. Keratinizing squamous cell carcinoma
- Type 2. Non keratinizing squamous cell carcinoma
- Type 3. Undifferentiated carcinoma ( the commonest)
Spread
- Direct spread.
- Lymphatic spread: to retropharyngeal LNs then to deep cervical LNs (early & common).
- Blood spread: to bone & lung (rare).
Nasopharyngeal cancer symptoms
In its very early stages, nasopharyngeal carcinoma is usually asymptomatic, but lately, symptoms of nasopharyngeal carcinoma may include:
- Appearance of a lump in the neck (80%): this is the most common symptom, occurs due to lymph node metastasis and it might be unilateral (on one side) or bilateral (occult primary), it is painless.
- Ear manifestations (73%): unilateral aural fullness, deafness, and referred otalgia due to recurrent ear infections resulting from Eustachian tube obstruction (direct extension of the tumor into the ear is also possible).
- Nasal manifestations (78%): nasal obstruction, usually unilateral, rarely bilateral and unilateral bloody discharge.
- Eye manifestations (about 25%): blurry or double vision, eye pain and squint due to infiltration of the 3rd, 4th and 6th cranial nerves.
- Face numbness due to infiltration of the 5th cranial nerve (early).
- Dysphagia (difficult swallowing), chocking and hoarseness of voice due to infiltration of the 9th and 10th cranial nerves.
- Weak shoulder elevation due to infiltration of the 11th cranial nerve.
- Dysartheria and tongue deviation to diseased side due to infiltration of the 12th cranial nerve.
- Headaches (61%)
All such symptoms already occur with many diseases other than nasopharyngeal cancer, so don't panic if you find out that you have one or more of the above symptoms, just consult your doctor.
Signs (Doctor examination)
Nasal endoscopy: nasopharyngeal reddish blood tinged mass or ulcer with hemorrhage and necrosis, most propably at the fossa of Rosenmüller..

Aural examination: secretory otitis media or acute otitis media, unilateral conductive hearing.
Cranial nerve examination: as described above.
Neck examination: Hard, fixed LNs at level 5 (posterior triangle)
The most common lymph nodes involved are the jugulodigastric, and upper and middle jugular nodes in the anterior cervical chain.

- Unilateral facial pain/ numbness.
- Unilateral palatal paralysis.
- Unilateral conductive hearing loss.
N.B. Trotter's triad (diagnostic of nasopharyngeal cancer)
Differential Diagnoses (DD) of Nasopharyngeal carcinoma
Doctors should exclude other diseases that cause similar clinical picture, such as:
- Pediatric Nasal Polyps
- Pediatric Rhabdomyosarcoma
- Pediatric Non-Hodgkin Lymphoma
Diagnosis of nasopharyngeal cancer
After taking detailed medical history, and doing full examination, E.N.T doctor may request some laboratory studies and investigations to confirm his diagnosis, these include:
- CT scan of the head and neck to detect tumor extension, cervical lymphadenopathy and erosion of skull base.
- CT chest: may be needed to detect distant metastases
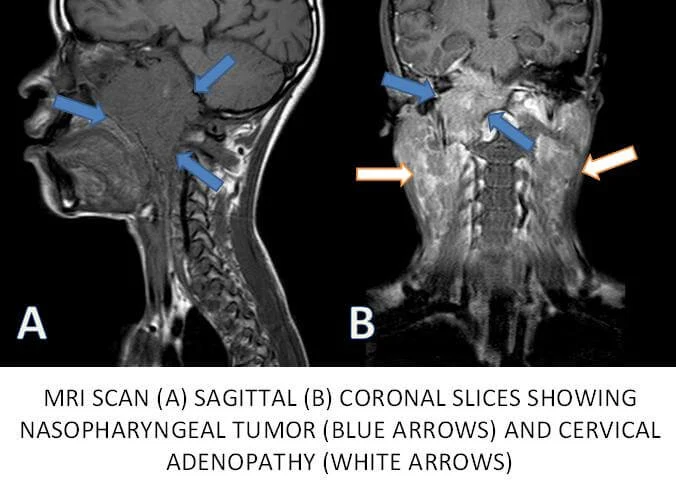
- MRI of the head and skull base: with intracranial extension and cranial nerve palsies.
- Endoscopic Biopsy & pathological examination (A biopsy is the removal of a small amount of tissue for examination under a microscope).
- Tympanogram type C or B.
- Metastatic work up: Bone scan, Positron emission tomography (PET).
Laboratory studies include:
- Epstein-Barr virus (EBV) titers: immunoglobulin A (IgA) and immunoglobulin G (IgG) antibodies to the viral capsid antigen.
- Complete blood count
- Liver function tests: AST, ALT, bilirubin, ...
- Creatinine clearance rates
Nasopharyngeal cancer staging
There are various schema suggested for staging of nasopharyngeal carcinoma in children.
No single system has proven satisfactory in correlating disease extent to its prognosis.
The staging system of the American Joint Committee on Cancer (AJCC) uses TNM scoring system, where T stands for "tumor", N stands for "Lymph Node" and M stands for "Metastasis".
a. Staging according to Tumor size and extention "T staging"
| Stage | Tumor extent |
|---|---|
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis | Carcinoma in situ |
| T1 | Tumor confined to the nasopharynx or extends to oropharynx and/or nasal cavity without parapharyngeal extension |
| T2 | Tumor with parapharyngeal extension |
| T3 | Tumor involves bony structures of skull base and/or paranasal sinuses |
| T4 | Tumor with intracranial extension and/or involvement of cranial nerves, hypopharynx, orbit, or with extension to the infratemporal fossa/masticator space |
b. Staging according to Lymph node envolvement "N staging"
| NX | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Unilateral metastasis in cervical lymph node(s), less than or equal to 6 cm in greatest dimension, above the supraclavicular fossa, and/or unilateral or bilateral retropharyngeal lymph nodes, less than or equal to 6 cm in greatest dimension |
| N2 | Bilateral metastasis in a cervical lymph node (s), less than or equal to 6 cm in greatest dimension, above the supraclavicular fossa |
| N3 | Metastasis in a lymph node(s) greater than 6 cm and/or to supraclavicular fossa |
| N3a | Greater than 6 cm in dimension |
| N3b | Extension to supraclavicular fossa |
c. M staging
| M0 | No distant metastasis |
| M1 | Distant metastasis |
Another simplified staging system
| Stage | Interpretation |
|---|---|
| Stage 0 | Carcinoma in situ |
| Stage 1 | Tumor has not spread to lymph nodes or distant parts of the body (early-stage nasopharyngeal cancer). |
| Stage 2 | Tumor spread to nearby tissues and lymph nodes but has not spread to distant parts of the body. |
| Stage 3 and stage 4 | More advanced because of tumor size, extent of spread to nearby tissues, lymph nodes, and/or distant parts of the body. |
| Recurrent cancer | when nasopharyngeal cancer returns after treatment. |
Nasopharyngeal cancer treatment and management
Treatment of nasopharyngeal carcinoma depends on many factors like location of the tumor, its stage and the general health condition of the patient.
a. Radiation Therapy
Radiotherapy is the best treatment option (with or without chemotherapy) for primary cases. Radiation therapy uses X-rays to kill cancer cells and stop them from growing.
Combination of radiotherapy with chemotherapy (cisplatin and 5-fluorouracil) usually improve survival rate according to recent studies espicially in locoregionally advanced nasopharyngeal carcinoma.
Some side effect may occur immediately with starting the course of radiotherapy (usually after 2 weeks) such as confluent mucositis, dry mouth, thick saliva. So, placement of a gastrostomy tube prior to initiation of radiotherapy is considered to prevent poor nutrition and dehydration.
IMRT (a type of radiation therapy) is known to apply high-dose radiation directly to the tumor while minimizing damage to nearby healthy tissue, that's why IMRT cuases fewer side effects or complications than conventional radiation.
b. Surgery
- Mostly, all tumors become unresectable at time of diagnosis because of their site (near nerves and blood vessels), and surgery is usually limited to biopsies for confirming diagnosis.
- Surgery may cause permanent damage to the eye and other nearby structures.
- Open surgical nasopharyngectomy: for recurrent or residual disease after radiotherapy / radiochemotherapy.
- Endoscopic nasopharyngectomy: recent technique for treatment of limited recurrent or residual disease after radiotherapy / radiochemotherapy.
c. Medications (Chemotherapy):
- Cisplatin and 5-fluorouracil have been shown to improve survival rates when cobined with radiotherapy.
- Nivolumab has been approved by the FDA for treatment of NPC since 2016, and it improved overall survival compared to classic medications.
d. Palliative treatment
- Palliative treatment aims at controling cancer symptoms and symptoms related to cancer treatment (side effects of therapy).
- Doctors suggest palliative therapy alone in cases where tumor has distant metastasis with little hope of cure.
- Palliation includes any procedure that relieves patient's suffering and pain (such as Anesthetic lozenges and sprays).
Prevention of Nasopharyngeal Cancer, is it possible?
Unfortunately, most cases of nasopharyngeal carcinoma are not preventable, but there are some precautions that may lower the risk of it, such as:
- Avoiding smoking (cessation if already a smoker)
- Avoiding Alcohol drinking
- Avoiding salt-cured fish and meats.
Nasopharyngeal cancer survival rate
Survival rate predicts the percentage of people with the same stage and type of cancer are still alive a certain amount of time (5 years usually).
| Tumor stage | 5-year relative survival rate |
|---|---|
| Localized | 82% |
| Regional | 73% |
| Distant | 48% |
| All of the above stages combined | 61% |
Interpretation
- Localized: There is no sign that the cancer has spread outside of the nasopharynx.
- Regional: The cancer has spread outside the nasopharynx to nearby structures or lymph nodes.
- Distant: The cancer has spread to distant parts of the body, such as the lungs or liver.
A relative survival rate compares people with the same type and stage of cancer to people in the overall population. For example, if the 5-year relative survival rate for a specific stage of nasopharyngeal cancer is 80%, it means that people who have that cancer are, on average, about 80% as likely as people who don’t have that cancer to live for at least 5 years after being diagnosed.
Recommended diet for patients with NPC
- Mashed potatoes, milkshakes, and pureed meats are advisable during the course of radiotherapy because they are soft and they don't irritate the mucosa of the nasopharynx.
- Avoid Citrus fruits, spicy foods, salty foods, and coarse foods because they irritate the mucose of the nasopharynx in patients with NPC who already have mucositis as a side effect of radiotherapy.
- In patients with severe mucositis, Gastrostomy tube placement should be considered.
Answers to FAQs about Nasopharyngeal Cancer
Q1. How do I know if I have nasopharyngeal cancer?
A. If you feel more than one of the above-mentioned symptoms, you should seek E.N.T specialist advice, you may need nasal endoscopy or other investigations determined by your doctor.
Q2. What is palliative care for nasopharyngeal cancer?
A. The main goal of palliative care is to make you feel as comfortable as possible and control your symptoms. It is for advanced cases (see staging above) where there is no cure.
Q3. Does everyone who get Epstein-Barr virus (EBV) get nasopharyngeal cancer?
A. NO. Having EBV infection doesn't mean that you will get nasopharyngeal cancer, it is just a predisposing factor.
Q4. Who gets nasopharyngeal cancer?
A. NPC is uncommon in the US (Less than one case/100000 people in North America). It is most common in southeast China. Other parts of Asia and North Africa have more cases than USA.
Q5. What increases the risk for nasopharyngeal cancer?
A. Eating diet rich in salt-cured fish and meat, and consumption of Tobacco and alcohol increse the risk of getting NPC, as chemicals in these stuff cause more damage to Cells' DNA.
Q6. When should I see my doctor about nasopharyngeal cancer?
If you have the above-mentioned symptoms, or some of them, please see your doctor as diagnosis (or ruling out) NPC needs doctor's experience.
References:
- WebMD Medical Reference Reviewed by Gabriela Pichardo on January 20, 2020
-American Cancer Society
-https://www.cancer.org/cancer/nasopharyngeal-cancer/detection-diagnosis-staging/survival-rates.html
-American Academy of Otolaryngology Head & Neck Surgery
-Cummings Otolaryngology Head & Neck Surgery, 4th edition
-Otorhinolaryngology for medical students (Cairo university, ENT department), second edition.