📋 Key Information Summary
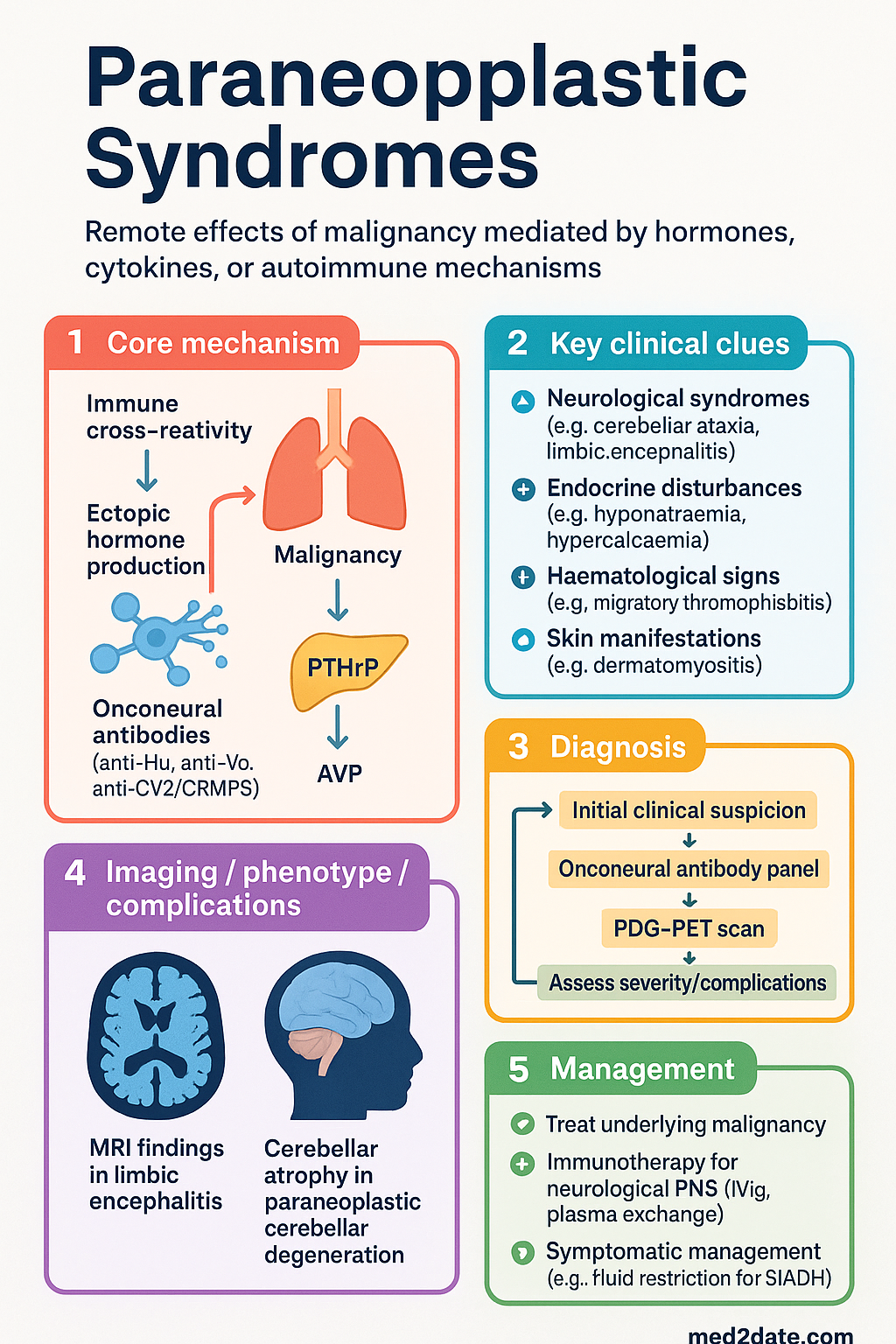
- Paraneoplastic syndromes (PNS) are remote effects of malignancy mediated by hormones, cytokines, or autoimmune mechanisms — not direct tumour invasion or metastasis.
- PNS may be the presenting feature of an occult malignancy; a high index of suspicion is critical for early cancer diagnosis.
- Endocrine PNS include SIADH (hyponatraemia in SCLC), ectopic ACTH syndrome, and malignancy-associated hypercalcaemia (PTHrP-mediated).
- Neurological PNS include Lambert-Eaton myasthenic syndrome (LEMS), paraneoplastic cerebellar degeneration, and limbic encephalitis — often associated with specific onconeural antibodies.
- Classic onconeural antibodies (anti-Hu, anti-Yo, anti-CV2/CRMP5, anti-amphiphysin) strongly suggest PNS even before cancer is detected.
- Haematological PNS include Trousseau syndrome (migratory thrombophlebitis), DIC, and erythrocytosis — thromboembolism may precede cancer diagnosis by months.
- Diagnosis requires exclusion of direct metastasis, infection, and treatment-related toxicity; onconeural antibody panels and FDG-PET are key investigations.
- Treatment of the underlying malignancy is the most effective strategy for PNS management.
- Immunotherapy (IVIg, plasma exchange, corticosteroids, rituximab) is indicated for most neurological PNS and some haematological PNS.
- Symptomatic management is essential: SIADH requires fluid restriction ± hypertonic saline; hypercalcaemia requires IV zoledronic acid or denosumab; seizures require anticonvulsants.
- Aboriginal and Torres Strait Islander peoples may present later with more advanced malignancy, increasing PNS risk; culturally safe pathways and remote telehealth access are essential.
- Venous thromboembolism (VTE) prophylaxis in cancer patients should follow Australian NHMRC and eviQ guidelines; unprovoked VTE in patients >40 years warrants occult malignancy screening.
- Some PNS (e.g., dermatomyositis, acanthosis nigricans maligna) have cutaneous manifestations detectable on physical examination — always examine the skin in suspected PNS.
Introduction & Australian Epidemiology
Paraneoplastic syndromes (PNS) are a heterogeneous group of clinical disorders associated with malignant disease that are not directly attributable to the physical effects of the primary tumour or its metastases. They are mediated by hormones, peptides, cytokines, or immune cross-reactivity between tumour antigens and normal tissues (onconeural antigens). PNS affect approximately 8–15% of patients with cancer and may be the earliest — and sometimes only — clinical manifestation of an otherwise occult malignancy.
Understanding PNS is critical for Australian clinicians across all disciplines, as early recognition can lead to timely cancer diagnosis, improved treatment outcomes, and prevention of irreversible organ damage. In the Australian context, the spectrum of cancers associated with PNS — particularly small-cell lung cancer (SCLC), breast carcinoma, ovarian carcinoma, thymoma, and haematological malignancies — mirrors global patterns, though regional variations in cancer incidence exist.
According to the Australian Institute of Health and Welfare (AIHW), lung cancer remains the fifth most common cancer in Australia (approximately 13,800 new diagnoses in 2023), with SCLC accounting for approximately 13% of cases. SCLC is the cancer most frequently associated with paraneoplastic endocrine syndromes. In Aboriginal and Torres Strait Islander peoples, lung cancer incidence is significantly higher (1.7× age-standardised rate) and is more often diagnosed at advanced stage, potentially increasing the burden of PNS.
The International Collaborative Group on PNS classification divides PNS into four broad categories: endocrine, neurological, haematological/vascular, and dermatological/musculoskeletal. This article follows a clinically oriented structure aligned with Australian practice.
Endocrine Paraneoplastic Syndromes
Endocrine PNS result from ectopic hormone production or inappropriate secretion of hormone-like peptides by tumour cells. These syndromes are often clinically apparent and may represent the initial presentation of an underlying malignancy.
Syndrome of Inappropriate Antidiuretic Hormone (SIADH)
SIADH is the most common endocrine PNS, occurring in approximately 10–15% of patients with small-cell lung cancer (SCLC). Ectopic production of arginine vasopressin (AVP) or AVP-like peptides by tumour cells leads to impaired free water excretion, dilutional hyponatraemia, and euvolaemic hypotonic hyponatraemia.
Diagnostic criteria for SIADH:
- Serum osmolality <275 mOsm/kg
- Urine osmolality >100 mOsm/kg
- Euvolaemic status (clinically)
- Urine sodium >40 mmol/L (with normal salt and water intake)
- Normal thyroid and adrenal function (must exclude hypothyroidism and adrenal insufficiency)
- No diuretic use
Ectopic ACTH Syndrome (Cushing Syndrome)
Ectopic ACTH production accounts for approximately 10–15% of all Cushing syndrome cases. SCLC, bronchial carcinoid, thymic carcinoid, medullary thyroid carcinoma, and phaeochromocytoma are the most common causes. The clinical presentation may differ from pituitary-dependent Cushing disease: hypokalaemic metabolic alkalosis, hyperpigmentation, rapid onset, and proximal myopathy are more prominent.
Malignancy-Associated Hypercalcaemia
Hypercalcaemia occurs in approximately 20–30% of patients with cancer during their illness. The three main mechanisms are: (1) PTHrP-mediated humoral hypercalcaemia of malignancy (HHM) — the most common, seen in squamous cell carcinomas, breast cancer, renal cell carcinoma; (2) osteolytic metastases with local cytokine release; and (3) 1,25-dihydroxyvitamin D production (lymphoma). HHM is characterised by suppressed PTH, elevated PTHrP, and often normal or low 1,25-vitamin D.
Neurological Paraneoplastic Syndromes
Neurological PNS are among the most clinically significant paraneoplastic conditions. They result from immune cross-reactivity between tumour-expressed onconeural antigens and the nervous system. Most are mediated by specific onconeural antibodies, though some (e.g., LEMS) involve direct antibody-mediated ion channel dysfunction rather than cytotoxic T-cell-mediated neuronal destruction.
Lambert-Eaton Myasthenic Syndrome (LEMS)
LEMS is an autoimmune presynaptic neuromuscular junction disorder caused by antibodies against P/Q-type voltage-gated calcium channels (VGCC). Approximately 60% of LEMS cases are paraneoplastic, overwhelmingly associated with SCLC. Clinical features include proximal limb weakness (especially lower limbs), autonomic dysfunction (dry mouth, constipation, erectile dysfunction), reduced or absent deep tendon reflexes that may "facilitate" with repeated testing, and a characteristic EMG pattern of incremental response to repetitive nerve stimulation (unlike myasthenia gravis).
Paraneoplastic Cerebellar Degeneration
Paraneoplastic cerebellar degeneration (PCD) presents with subacute onset of severe truncal and limb ataxia, dysarthria, nystagmus, and often cognitive changes. It may be associated with anti-Yo antibodies (breast, ovarian cancer), anti-Tr/DNER (Hodgkin lymphoma), anti-Hu (SCLC), or anti-CV2/CRMP5 (SCLC, thymoma). Brain MRI may initially appear normal but shows progressive cerebellar atrophy over weeks to months.
PCD associated with classic onconeural antibodies is largely resistant to immunotherapy due to irreversible Purkinje cell loss. However, aggressive tumour treatment (surgery, chemotherapy) may stabilise or modestly improve neurological function in some patients.
Paraneoplastic Limbic Encephalitis
Paraneoplastic limbic encephalitis (PLE) is characterised by subacute onset of short-term memory loss, seizures, psychiatric symptoms (anxiety, depression, psychosis), and temporal lobe abnormalities on MRI (increased T2/FLAIR signal in mesial temporal structures). It may be associated with:
- Anti-Hu: SCLC — aggressive, poor prognosis
- Anti-Ma2: Testicular germ cell tumour — may also cause brainstem encephalitis
- Anti-NMDAR: Ovarian teratoma — especially in young women; better prognosis if tumour removed
- Anti-CASPR2 / anti-LGI1: Thymoma — may be non-paraneoplastic in older males
Paraneoplastic Neuropathies
Subacute sensory neuronopathy (anti-Hu-associated) is the classic paraneoplastic neuropathy. It presents with asymmetric, predominantly sensory neuropathy with sensory ataxia, pseudoathetosis, and often preserved motor function. It is most commonly associated with SCLC and tends to be severe and treatment-resistant. Dorsal root ganglion inflammation is the pathological hallmark.
Other paraneoplastic neuropathies include autonomic neuropathy (anti-ganglionic AChR antibodies), sensorimotor axonal neuropathy, and demyelinating neuropathies resembling CIDP. Autonomic neuropathy with anti-ganglionic AChR antibodies may present with severe gastrointestinal dysmotility (intestinal pseudo-obstruction), orthostatic hypotension, and anhidrosis.
Paraneoplastic Opsoclonus-Myoclonus Syndrome (OMS)
OMS (dancing eyes–dancing feet syndrome) is characterised by rapid, involuntary, multidirectional saccades (opsoclonus), myoclonus, ataxia, and behavioural changes. In paediatric patients, it is associated with neuroblastoma (50% of cases); in adults, SCLC and breast cancer. In children, OMS may be the presenting feature of otherwise clinically occult neuroblastoma, and urinary catecholamines (HVA, VMA) and MIBG scanning are essential investigations.
Haematological & Other Syndromes
Haematological PNS encompass a range of blood count abnormalities and coagulation disorders that arise as a consequence of malignancy through mechanisms separate from direct marrow infiltration.
Trousseau Syndrome (Cancer-Associated Thrombosis)
Trousseau syndrome describes migratory superficial thrombophlebitis and a hypercoagulable state associated with occult malignancy. Venous thromboembolism (VTE) — including deep vein thrombosis (DVT), pulmonary embolism (PE), and unusual-site thrombosis (portal vein, cerebral sinuses, upper limb) — may be the presenting feature of cancer, preceding the cancer diagnosis by months. Pancreatic, lung, gastric, and ovarian cancers carry the highest risk.
Management of cancer-associated VTE:
Paraneoplastic Erythrocytosis
Ectopic erythropoietin (EPO) production causes paraneoplastic erythrocytosis, most commonly associated with renal cell carcinoma, hepatocellular carcinoma, cerebellar haemangioblastoma, and uterine fibroids. Serum EPO levels are inappropriately elevated for the haematocrit. Management is directed at treating the underlying tumour; phlebotomy is rarely needed.
Paraneoplastic Eosinophilia
Marked peripheral eosinophilia may occur with T-cell lymphomas (mycosis fungoides, Sézary syndrome), Hodgkin lymphoma, and solid tumours. Eosinophilic infiltration of tissues (skin, lungs, heart) may cause organ damage. IL-5 secretion by the tumour is the typical mechanism.
Paraneoplastic Autoimmune Cytopenias
Autoimmune haemolytic anaemia (AIHA), immune thrombocytopenia (ITP), and pure red cell aplasia (PRCA) may be associated with lymphoproliferative disorders (CLL, non-Hodgkin lymphoma) and thymoma. Warm AIHA is treated with corticosteroids (prednisolone 1 mg/kg/day) as first-line; refractory cases may require rituximab (375 mg/m² IV weekly × 4) or splenectomy. PRCA with thymoma often resolves after thymectomy.
Dermatological Paraneoplastic Syndromes
Dermatological manifestations may provide important diagnostic clues:
- Dermatomyositis: Heliotrope rash, Gottron papules, proximal myopathy — associated with ovarian, lung, gastric, and nasopharyngeal cancers (particularly relevant in the Australian–Asian population)
- Acanthosis nigricans maligna: Sudden onset, extensive, pruritic — associated with gastric adenocarcinoma
- Paraneoplastic pemphigus: Severe mucocutaneous blistering — associated with CLL, Castleman disease, NHL
- Sweet syndrome (acute febrile neutrophilic dermatosis): Painful erythematous plaques, neutrophilia — associated with haematological malignancies
- Erythema gyratum repens: Wood-grain pattern migratory erythema — high association with lung and oesophageal cancer
Diagnosis & Management
The diagnosis of PNS requires a systematic approach integrating clinical assessment, serological testing, imaging, and exclusion of alternative diagnoses. The European PNS Euronetwork diagnostic criteria remain widely used.
Diagnostic Approach
Investigations Summary
Treatment Principles
Monitoring
Monitoring in PNS involves both oncological and neurological/systematic assessment:
- Repeat onconeural antibody titres every 3–6 months (may correlate with clinical status in some PNS, though classic antibodies may remain elevated despite treatment)
- Serial neurological examination and disability scoring (mRankin, EDSS where appropriate)
- Repeat FDG-PET/CT at 3–6 months if initial cancer screening negative (approximately 10–20% of patients develop detectable cancer within 2–5 years)
- Endocrine monitoring: serum sodium every 4–6 hours during SIADH treatment; serum calcium every 2–3 days during hypercalcaemia management; cortisol levels for ectopic ACTH
- VTE surveillance in cancer patients: clinical assessment at each visit; imaging if new symptoms
- Ongoing cancer surveillance for minimum 2–5 years in patients with onconeural antibodies but no detectable malignancy at initial workup
ATSI (Aboriginal and Torres Strait Islander) Health Considerations
Quick Reference: Cancer–Antibody–Syndrome Associations
| Antibody | Syndrome | Associated Cancer | Prognosis |
|---|---|---|---|
| Anti-Hu (ANNA-1) | Sensory neuronopathy, limbic encephalitis, cerebellar degeneration | SCLC | Poor; irreversible neuronal loss |
| Anti-Yo (PCA-1) | Cerebellar degeneration | Breast, ovarian | Poor; Purkinje cell loss |
| Anti-CV2/CRMP5 | Cerebellar, neuropathy, uveitis | SCLC, thymoma | Variable |
| Anti-amphiphysin | Stiff-person syndrome, neuropathy | SCLC, breast | Poor |
| Anti-Ma2 | Limbic/brainstem encephalitis | Testicular germ cell | Moderate (if tumour treated) |
| Anti-P/Q-VGCC | LEMS | SCLC | Moderate–good |
| Anti-NMDAR | Limbic encephalitis | Ovarian teratoma | Good (with tumour removal) |
| Anti-Tr/DNER | Cerebellar degeneration | Hodgkin lymphoma | Moderate |
| Anti-Ri (ANNA-2) | Opsoclonus-myoclonus, ataxia | Breast, SCLC | Variable |
Australian Referral Pathways
Paraneoplastic syndromes require a multidisciplinary approach:
- Neurology: All suspected neurological PNS — urgent referral for antibody testing, CSF analysis, electrophysiology, and immunotherapy initiation
- Medical Oncology: Cancer diagnosis, staging, and tumour-directed therapy; coordination with PNS management
- Endocrinology: SIADH, ectopic ACTH, and hypercalcaemia management; hormone-directed therapy
- Haematology: Cancer-associated thrombosis, paraneoplastic cytopenias, DIC management
- Dermatology: Suspected dermatological PNS (dermatomyositis, pemphigus) — skin biopsy + cancer screening
- General Practice: Ongoing surveillance (repeat cancer screening if initial negative), VTE prophylaxis coordination, chronic disease management, ATSI health check coordination
- Radiology: FDG-PET/CT (eviQ referral guidelines), CT guided biopsy for occult lesions
📚 References
- 1. Graus F, Delattre JY, Antoine JC, et al. Recommended diagnostic criteria for paraneoplastic neurological syndromes. J Neurol Neurosurg Psychiatry. 2004;75(8):1135–1140.
- 2. Giometto B, Grisold W, Vitaliani R, et al. Paraneoplastic neurological syndrome in the PNS Euronetwork database. Arch Neurol. 2010;67(3):330–335.
- 3. Titulaer MJ, Soffietti R, Dalmau J, et al. Screening for tumours in paraneoplastic syndromes: report of an EFNS Task Force. Eur J Neurol. 2011;18(1):19–e3.
- 4. Dalmau J, Gleichman AJ, Hughes EG, et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies. Lancet Neurol. 2008;7(12):1091–1098.
- 5. Titulaer MJ, McCracken L, Gabilondo I, et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. 2013;12(2):157–165.
- 6. Titulaer MJ, Lang B, Verschuuren JJ. Lambert-Eaton myasthenic syndrome: from clinical characteristics to therapeutic strategies. Lancet Neurol. 2011;10(12):1098–1107.
- 7. Australian Institute of Health and Welfare. Cancer data in Australia. AIHW, Canberra. 2023. Available from: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia
- 8. National Health and Medical Research Council. Australian guidelines for the prevention and management of venous thromboembolism. NHMRC, Canberra. 2009 (updated 2021).
- 9. Cancer Institute NSW. eviQ Cancer Treatments Online: venous thromboembolism in cancer. Available from: https://www.eviq.org.au/
- 10. Vedeler CA, Antoine JC, Giometto B, et al. Management of paraneoplastic neurological syndromes: report of an EFNS Task Force. Eur J Neurol. 2006;13(7):682–690.
- 11. Rosenfeld MR, Dalmau J. Diagnosis and management of paraneoplastic neurological disorders. Curr Treat Options Oncol. 2013;14(4):528–538.
- 12. Conner SE, Lorusso D, Bhola P, et al. Paraneoplastic syndromes in Aboriginal and Torres Strait Islander Australians: barriers to diagnosis and management. Aust J Rural Health. 2022;30(4):478–485.
- 13. Rogiers A, Leys C, De Cremer J, et al. Targeting intracellular versus extracellular onconeural antigens in paraneoplastic neurological syndromes: a systematic review. Neuro-Oncology Advances. 2023;5(1):vdac185.
- 14. Lee JW, Jeon HJ, Sun DI, Kim MJ. Cancer-related hypercalcemia: a review of current approaches to diagnosis and treatment. Korean J Intern Med. 2023;38(3):301–314.