📋 Key Information Summary
- Colorectal cancer (CRC) is the third most commonly diagnosed cancer and the second leading cause of cancer-related death in Australia.
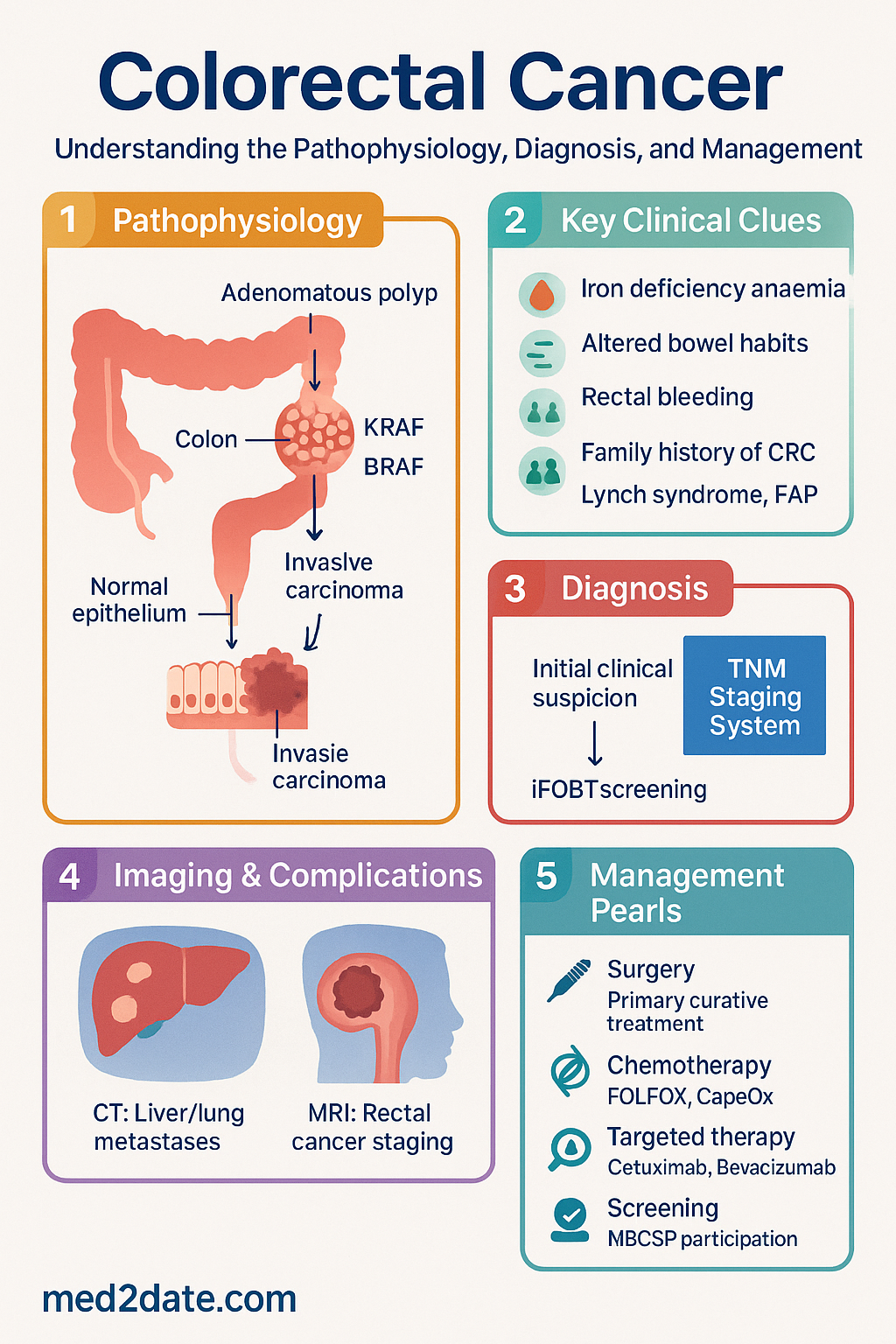
- Over 95% are adenocarcinomas, arising from the malignant transformation of adenomatous polyps over 10–15 years.
- Key modifiable risk factors include high consumption of red/processed meat, obesity, smoking, and excessive alcohol intake.
- Non-modifiable risk factors include age >50, inflammatory bowel disease (IBD), and inherited syndromes like Lynch syndrome (HNPCC) and Familial Adenomatous Polyposis (FAP).
- The Australian National Bowel Cancer Screening Program (NBCSP) uses immunochemical faecal occult blood testing (iFOBT) for population screening from age 50.
- Diagnosis is confirmed by colonoscopy and histological biopsy. Essential staging investigations include CT chest/abdomen/pelvis and MRI pelvis for rectal cancer.
- Treatment is stage-dependent and guided by multidisciplinary team (MDT) discussion. Surgery is the primary curative treatment for localised disease.
- For locally advanced rectal cancer, neoadjuvant chemoradiotherapy (e.g., 5-FU/capecitabine + radiation) is standard to improve resectability and local control.
- Adjuvant chemotherapy (e.g., FOLFOX, CapeOx) is indicated for stage III and high-risk stage II colon cancer.
- For metastatic disease, treatment intent (curative vs. palliative) and RAS/BRAF mutation status guide the use of targeted agents like cetuximab, bevacizumab, and encorafenib.
- Aboriginal and Torres Strait Islander peoples have higher CRC incidence and mortality, with later presentation and greater barriers to optimal care.
Introduction & Australian Epidemiology
Colorectal cancer (CRC) encompasses malignancies of the colon and rectum. It is a major cause of cancer morbidity and mortality in Australia, with a lifetime risk of approximately 1 in 13 for both sexes. The disease typically arises through the adenoma-carcinoma sequence, a stepwise progression from normal epithelium to adenomatous polyp to invasive carcinoma, driven by the accumulation of genetic and epigenetic alterations.
In Australia, CRC is the third most common cancer (excluding non-melanoma skin cancers) and the second most common cause of cancer death. According to the Australian Institute of Health and Welfare (AIHW), an estimated 15,500 new cases are diagnosed annually. Incidence increases sharply with age, with the majority of cases diagnosed in those over 50. Mortality rates have been gradually declining due to screening, improved treatments, and earlier detection. Significant disparities exist, with Aboriginal and Torres Strait Islander peoples experiencing poorer outcomes.
Epidemiology & Risk Factors
Incidence and Trends
Age-standardised incidence rates are around 58 per 100,000 population. Incidence is slightly higher in males. While overall rates are stable or declining in those over 50, possibly due to screening, there is a concerning rise in early-onset CRC (diagnosed under 50) for reasons not yet fully understood.
Risk Factors
- Non-modifiable: Age >50 years (strongest risk factor), male sex, personal history of CRC or adenomas, inflammatory bowel disease (ulcerative colitis, Crohn's colitis), family history of CRC in first-degree relatives, and hereditary syndromes (Lynch syndrome, FAP, MUTYH-associated polyposis).
- Modifiable: Diet high in red and processed meats, low fibre intake, obesity (particularly central adiposity), physical inactivity, smoking, and heavy alcohol consumption.
- Protective Factors: Regular physical activity, aspirin/NSAID use (in specific high-risk contexts after medical consultation), and a diet rich in fruits, vegetables, and whole grains.
Australian Screening
The Australian National Bowel Cancer Screening Program (NBCSP) mails iFOBT kits to all eligible Australians aged 50–74 every two years. A positive iFOBT mandates follow-up colonoscopy. Participation rates remain suboptimal (~40%), particularly in lower socioeconomic and regional/remote populations.
Pathology & TNM Staging
Histopathology
The vast majority (>95%) of colorectal cancers are adenocarcinomas. Key pathological features reported include: histological subtype (e.g., mucinous, signet ring cell), grade of differentiation, depth of invasion (pT stage), lymphovascular invasion, perineural invasion, and the number of lymph nodes examined (ideally ≥12).
Molecular Pathology
Essential molecular testing for all metastatic CRC includes:
- RAS (KRAS/NRAS) mutation status: Predicts resistance to anti-EGFR therapies (cetuximab, panitumumab). Approximately 45% of CRCs harbour a KRAS mutation.
- BRAF V600E mutation status: Indicates a very poor prognosis. Present in ~8-10% of cases. It is also a hallmark of sporadic microsatellite instability-high (MSI-H) tumours.
- Microsatellite Instability (MSI) / Mismatch Repair (MMR) deficiency: Tested by immunohistochemistry (IHC) for MMR proteins (MLH1, MSH2, MSH6, PMS2) or PCR. MSI-H/dMMR tumours (15% of stage II/III) have a better prognosis in early-stage disease and predict benefit from immune checkpoint inhibitors (e.g., pembrolizumab) in the metastatic setting.
TNM Staging (AJCC/UICC 8th Edition)
| Stage | T (Tumour) | N (Nodes) | M (Metastasis) | Description |
|---|---|---|---|---|
| 0 | Tis | N0 | M0 | Carcinoma in situ (high-grade dysplasia) |
| I | T1-T2 | N0 | M0 | Tumour invades submucosa (T1) or muscularis propria (T2) |
| IIA/B/C | T3/T4a/T4b | N0 | M0 | Tumour invades through muscularis propria into pericolorectal tissues/serosa (T3) or perforates/invades adjacent structures (T4) |
| IIIA/B/C | Any T | N1/N2 | M0 | Metastasis to 1-3 (N1) or ≥4 (N2) regional lymph nodes |
| IVA/B/C | Any T | Any N | M1a/b/c | Distant metastasis: single organ (M1a), multiple organs (M1b), peritoneal metastasis +/- other sites (M1c) |
Clinical Features & Investigations
Clinical Presentation
Symptoms depend on tumour location and stage. Right-sided (ascending) colon cancers often present insidiously with iron deficiency anaemia, fatigue, and occult blood loss. Left-sided (descending/sigmoid) and rectal cancers typically present with altered bowel habit, rectal bleeding, tenesmus, or symptoms of obstruction. Acute presentations include bowel obstruction or, rarely, perforation. Constitutional symptoms (weight loss, anorexia) often indicate advanced disease.
Investigations
Treatment (Surgery, Chemotherapy & Targeted Therapy)
All patients should be discussed at a specialist multidisciplinary team (MDT) meeting. Treatment is stage-dependent.
Surgery
The mainstay of curative treatment for non-metastatic disease. The goal is a complete oncological resection with clear margins (≥5 mm for colon, ≥1 mm for rectum).
- Colon Cancer: Segmental colectomy (e.g., right hemicolectomy, sigmoid colectomy) with high ligation of the vascular pedicle and en-bloc lymphadenectomy (≥12 nodes). Laparoscopic surgery is standard where feasible.
- Rectal Cancer: Total Mesorectal Excision (TME) is the standard. Surgery type (anterior resection with colo-anal anastomosis, or abdominoperineal excision) depends on tumour height relative to the anal sphincter. For early T1 tumours, transanal endoscopic microsurgery (TEM) may be appropriate.
- Emergency Surgery: Required for obstruction or perforation. May involve stent placement (bridge to surgery) or a Hartmann's procedure.
Chemotherapy & Targeted Therapy
Pharmacotherapy is used in the adjuvant (post-surgery) and metastatic settings. All regimens below are intravenous unless stated. Dose adjustments are mandatory for renal/hepatic impairment, elderly, or poor performance status.
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a greater burden from colorectal cancer, characterised by higher incidence in some age groups, significantly higher mortality rates (approx. 1.5x), and later stage at diagnosis. This inequity is driven by systemic and socio-economic barriers.
📚 References
- 1. Cancer Council Australia. Clinical practice guidelines for the prevention, early detection and management of colorectal cancer. Sydney: Cancer Council Australia; 2017. Available from: https://wiki.cancer.org.au/australia/Clinical_guidelines
- 2. Australian Institute of Health and Welfare (AIHW). Cancer data in Australia. Cat. no. CAN 122. Canberra: AIHW; 2023.
- 3. Department of Health. National Bowel Cancer Screening Program. Australian Government. Accessed 2024.
- 4. Amin MB, Edge SB, Greene FL, et al., editors. AJCC Cancer Staging Manual. 8th ed. New York: Springer; 2017.
- 5. National Health and Medical Research Council (NHMRC). Australian guidelines for the prevention and management of pressure injuries. Canberra: NHMRC; 2024. [Relevance: Surgical care standards]
- 6. Cancer Council Australia Colorectal Cancer Guidelines Working Party. Investigation and surgical management of colorectal cancer. In: Cancer Council Australia Clinical Guidelines Network. [Updated 2023].
- 7. Pharmac Benefits Scheme (PBS). Schedule of Pharmaceutical Benefits. Australian Government Department of Health. Accessed 2024.
- 8. National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Colon Cancer. Version 2.2024.
- 9. Conroy T, Bosset JF, Etienne PL, et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(5):702-715.
- 10. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander health performance framework 2023 summary report. Canberra: AIHW; 2023.
- 11. Royal Australasian College of Surgeons (RACS). Standards for the management of colorectal cancer. Melbourne: RACS; 2020.
- 12. André T, Shiu KK, Kim TW, et al. Pembrolizumab in Microsatellite-Instability–High Advanced Colorectal Cancer. N Engl J Med. 2020;383(23):2207-2218.