In this article , we are going to discuss the incidence and clinical manifestations of Rheumatoid arthritis (symptoms and signs and clinical course), illustrating common deformities that R.A can cause to joints , taking in consideration the Extra-articular manifestations.
-For def. , causes and pathology of R.A : click here
Incidence
• Female : Male ratio ( 3 : 1 ) it usually occurs at age 30-40 years, but it can occur at any age from 10-70 years.
• It affects 1% of population.

• Acute polyarthritis + fever + leucocytosis.
• Acute monoarthritis as rheumatic fever.
• Chronic monoarthritis (Insidious painful swelling of a large joint).
• Soft tissue lesions
- Tenosynovitis.
- Carpal tunnel $.
• Typical onset which is gradual and slowly progressive, Symmetrical polyarthritis affecting small joint of the hands, feet and wrist (the commonest).
• Palindromic onset with recurrent acute episodes of joint pain and stiffness for 24-48 hours, 50% progress to other types of RA.
• Painful, swollen, stiff joints (mainly of the hands and feet) .
• Effusion in large joints may occur.
• Morning stiffness (duration is an index of activity, it decreases towards end of the day).
The affected Joints (symmetrical arthropathy) :
1- Hands
- Proximal interphalangeal joint.
- Metacarpophalangeal joint.
(The distal interphalangeal joints are usually spared)
Common deformities :-
• Ulnar deviation of Metcarpo-phalangeal joint due to sublaxation.
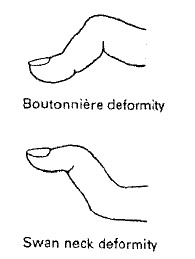 • Swan Neck deformity (flexion of the distal inter-phalangeal joint and hyperextension of proximal inter phalangeal joint).
• Swan Neck deformity (flexion of the distal inter-phalangeal joint and hyperextension of proximal inter phalangeal joint).
• Boutoniere deformity : flexion of proximal inter phalangeal joint and hyperextension of distal inter phalangeal joint) .
• Trigger finger : inability to extend finger at metcarpophalangeal joint .(tenosynovitis with nodules of flexor tendons) causes intermittent
locking of the finger in flexion.
• Z deformity of the tumb (Hyperextension of the interphalangeal joint and flexion of the metcarpo-phalangeal joint).
2- Wrists : subluxation may occur.
3- Feet
• Metatarsophalangeal and inter phalangeal arthritis.
• Achilies tendinitis.
4- Elbows
5- Cervical spine : atlanto-axial sublaxation with cord compression producing pyramidal and sensory signs. Atlanto-axial sublaxation should be suspected in any patient with R.A complaining of new onset of occipital headache .
6- Knee
• Progressive flexion deformity.
• Inflammation with hypertrophy or effusion of the bursa of calf and semi membranous muscle ---> Baker's cyst (tender swelling of popliteal fossa).
7- Tempromandibular joint is: - Painful. - Tender.
8- Other joints e.g. acromioclavicular, sternoclavicular, cricoarytenoied can be affected.
9- Other musculoskeletal manifestations e.g Bursitis, periarticular osteoporosis, disuse muscle wasting especially the small muscle of the
hand.
-For def. , causes and pathology of R.A : click here
Incidence
• Female : Male ratio ( 3 : 1 ) it usually occurs at age 30-40 years, but it can occur at any age from 10-70 years.
• It affects 1% of population.
Mode of onset

• Acute monoarthritis as rheumatic fever.
• Chronic monoarthritis (Insidious painful swelling of a large joint).
• Soft tissue lesions
- Tenosynovitis.
- Carpal tunnel $.
• Typical onset which is gradual and slowly progressive, Symmetrical polyarthritis affecting small joint of the hands, feet and wrist (the commonest).
• Palindromic onset with recurrent acute episodes of joint pain and stiffness for 24-48 hours, 50% progress to other types of RA.
So,what is the clinical course of Rheumatoid arthritis ?
It is usually life-long with intermittent remissions and exacerbationsI- Musculoskeletal manifestations
• Painful, swollen, stiff joints (mainly of the hands and feet) .
• Effusion in large joints may occur.
• Morning stiffness (duration is an index of activity, it decreases towards end of the day).
The affected Joints (symmetrical arthropathy) :
1- Hands
- Proximal interphalangeal joint.
- Metacarpophalangeal joint.
(The distal interphalangeal joints are usually spared)
Common deformities :-
• Ulnar deviation of Metcarpo-phalangeal joint due to sublaxation.
 • Swan Neck deformity (flexion of the distal inter-phalangeal joint and hyperextension of proximal inter phalangeal joint).
• Swan Neck deformity (flexion of the distal inter-phalangeal joint and hyperextension of proximal inter phalangeal joint).• Boutoniere deformity : flexion of proximal inter phalangeal joint and hyperextension of distal inter phalangeal joint) .
• Trigger finger : inability to extend finger at metcarpophalangeal joint .(tenosynovitis with nodules of flexor tendons) causes intermittent
locking of the finger in flexion.
• Z deformity of the tumb (Hyperextension of the interphalangeal joint and flexion of the metcarpo-phalangeal joint).
2- Wrists : subluxation may occur.
3- Feet
• Metatarsophalangeal and inter phalangeal arthritis.
• Achilies tendinitis.
4- Elbows
5- Cervical spine : atlanto-axial sublaxation with cord compression producing pyramidal and sensory signs. Atlanto-axial sublaxation should be suspected in any patient with R.A complaining of new onset of occipital headache .
6- Knee
• Progressive flexion deformity.
• Inflammation with hypertrophy or effusion of the bursa of calf and semi membranous muscle ---> Baker's cyst (tender swelling of popliteal fossa).
7- Tempromandibular joint is: - Painful. - Tender.
8- Other joints e.g. acromioclavicular, sternoclavicular, cricoarytenoied can be affected.
9- Other musculoskeletal manifestations e.g Bursitis, periarticular osteoporosis, disuse muscle wasting especially the small muscle of the
hand.