📋 Key Information Summary
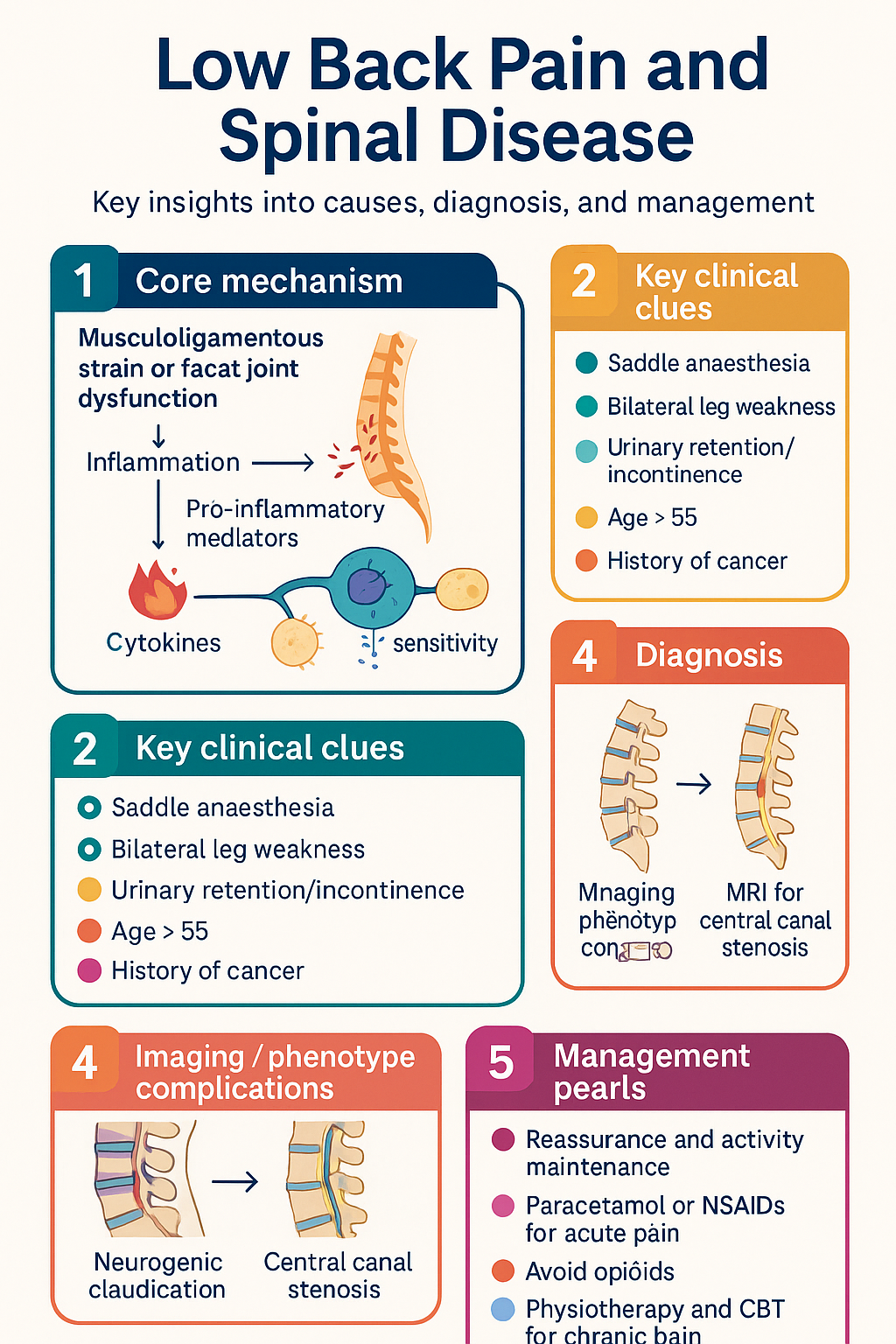
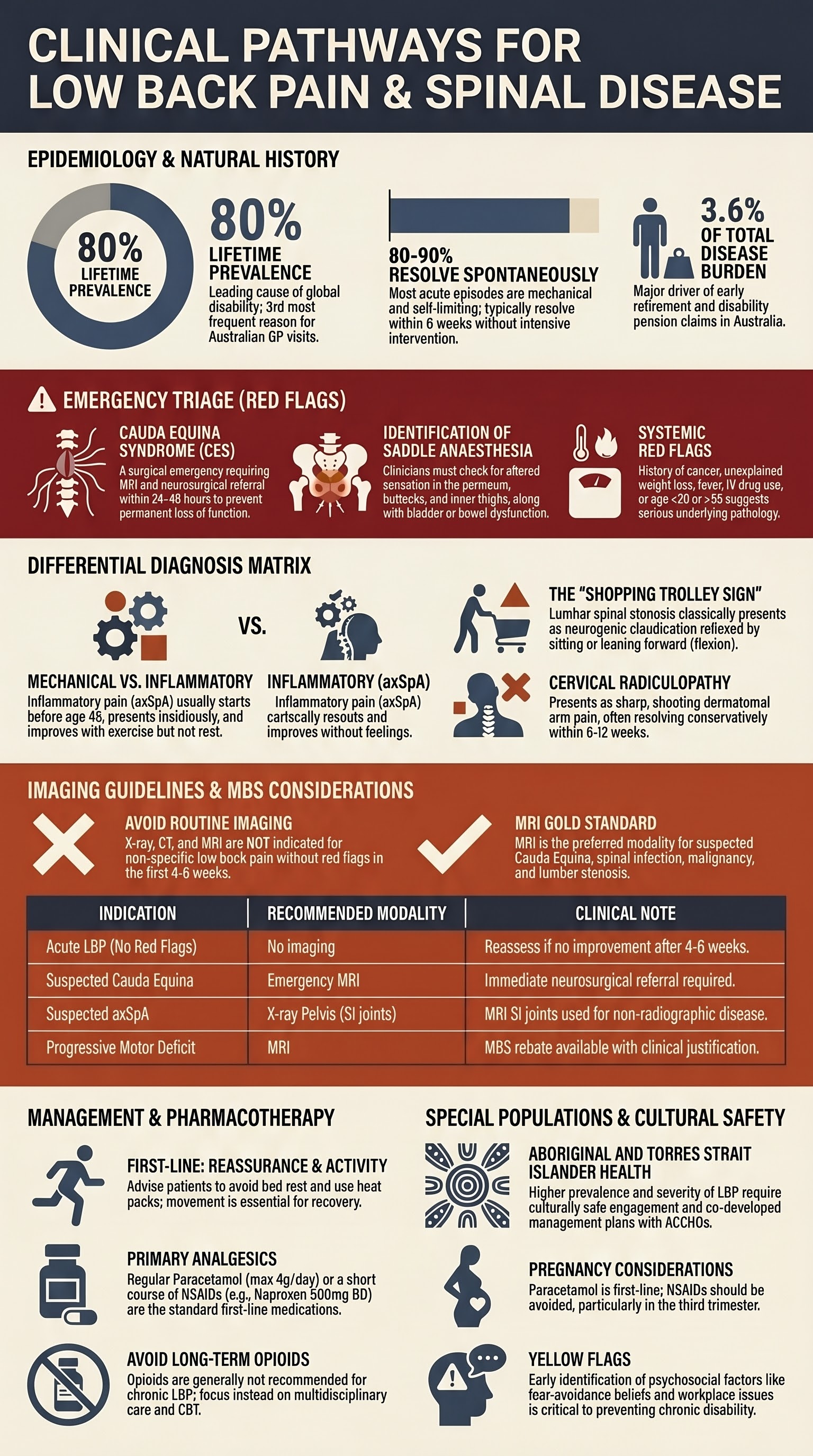
- Most acute low back pain is mechanical and self-limiting (80-90% resolve within 6 weeks). Reassurance and maintaining activity are first-line.
- Cauda equina syndrome (saddle anaesthesia, bilateral leg weakness, urinary retention/incontinence) is a surgical emergency requiring urgent MRI and neurosurgical referral.
- Red flags for serious pathology include: age <20 or >55, history of cancer, unexplained weight loss, fever, IV drug use, prolonged corticosteroid use, and failure to improve after 4-6 weeks.
- Routine imaging (X-ray, CT, MRI) is NOT indicated for non-specific low back pain without red flags in the first 4-6 weeks.
- Inflammatory back pain (axSpA) is suggested by: age <45, insidious onset, improvement with exercise, no improvement with rest, and night pain. Refer to rheumatology for HLA-B27 and MRI sacroiliac joints.
- Lumbar spinal stenosis classically causes neurogenic claudication: bilateral leg pain/numbness worsened by standing/walking and relieved by sitting/flexion (the "shopping trolley sign").
- Cervical radiculopathy typically presents with dermatomal arm pain, numbness, and weakness. Most cases improve with conservative management (physiotherapy, short-term analgesics).
- For acute mechanical LBP, first-line pharmacotherapy is regular paracetamol or an NSAID (e.g., naproxen) for a short course. Avoid opioids if possible.
- Multidisciplinary pain programmes are key for chronic non-specific LBP (>3 months). Focus on active therapies (exercise, CBT) over passive therapies.
- Aboriginal and Torres Strait Islander peoples experience higher rates of spinal disease, later presentation, and barriers to specialist care. Culturally safe engagement is essential.
- Consider psychosocial factors (yellow flags) early: fear-avoidance beliefs, catastrophising, and workplace issues. These are strong predictors of chronicity.
Introduction & Australian Epidemiology
Low back pain (LBP) is the leading cause of disability worldwide and a major burden on the Australian healthcare system. Lifetime prevalence is approximately 80%. It is the third most common reason for consulting a GP in Australia. Most episodes are non-specific and mechanical in origin, with a favourable natural history. However, it is a significant driver of work absenteeism, healthcare costs, and long-term opioid use.
This guideline covers key spinal conditions presenting with back and neck pain, emphasising a biopsychosocial model, appropriate investigation, and management within the Australian context. The focus is on early identification of serious pathology, rational use of imaging, and evidence-based conservative care.
Mechanical Low Back Pain
Clinical Presentation & Diagnosis
Pain is localised to the lumbosacral region, with or without leg pain (non-radicular). It is typically worsened by movement and load, and relieved by rest. Examination findings are non-specific, with possible paraspinal tenderness and limited range of motion. Neurological exam (straight leg raise, dermatomes, myotomes) should be normal.
Pathophysiology
Often attributed to musculoligamentous strain or facet joint dysfunction, but a specific anatomical source is rarely identifiable. Degenerative changes (disc bulges, facet arthrosis) on imaging are common in asymptomatic individuals and correlate poorly with symptoms.
Management
First-line: Reassurance about good prognosis, advice to remain active, and self-care (heat pack). Avoid bed rest.
Second-line / Chronic pain: Consider duloxetine (PBS Authority Required for chronic musculoskeletal pain) or short-course muscle relaxants (e.g., diazepam 2-5 mg nocte, max 7 days). Opioids are generally not recommended for chronic LBP.
Non-pharmacological: Referral for physiotherapy (exercise-based), massage, or chiropractic care for persistent symptoms. CBT for chronic pain with significant psychosocial contributors.
Lumbar Spinal Stenosis
Clinical Presentation
Neurogenic claudication: bilateral or unilateral leg pain, heaviness, numbness, or weakness provoked by standing or walking, and relieved by sitting or spinal flexion (the "shopping trolley sign"). Symptoms often improve when pushing a supermarket trolley. Examination may be normal between episodes; calf wasting or mild weakness may be present.
Diagnosis
Clinical diagnosis supported by imaging. MRI lumbar spine is the gold standard to confirm central canal stenosis and exclude other pathologies. See Imaging Guidelines section.
Management
Conservative (first-line): Supervised physiotherapy (flexion-based exercises, core stability), weight loss, walking aids. Gabapentinoids (e.g., pregabalin) may help neuropathic leg pain.
Surgical referral: Indicated for progressive neurological deficit, severe symptoms refractory to 3-6 months of conservative care, or significant impact on quality of life. Decompressive laminectomy has good outcomes for appropriately selected patients.
Cervical Radiculopathy
Clinical Presentation
Sharp, shooting pain radiating down the arm in a dermatomal pattern, often with associated numbness, paraesthesia, or weakness. Coughing or sneezing may exacerbate pain. Common levels: C6 (thumb, biceps weakness), C7 (middle finger, triceps weakness). Spurling's test may be positive.
Diagnosis & Differential
Primarily clinical. Differentiate from carpal tunnel syndrome, rotator cuff pathology, or Pancoast tumour. MRI cervical spine is indicated if symptoms persist >6 weeks or with progressive neurological deficit.
Management
Most cases (75-90%) improve with conservative care within 6-12 weeks.
- Analgesia: NSAIDs, simple analgesics. Short course of oral corticosteroids (e.g., prednisone 50 mg daily for 5 days) may reduce acute radicular pain.
- Physiotherapy: Cervical traction, postural advice, and nerve gliding exercises.
- Referral: To neurosurgery or orthopaedic spine surgery for: progressive motor weakness, intractable pain, or signs of myelopathy (e.g., gait disturbance, hyperreflexia, upgoing plantars).
Inflammatory Back Pain & Axial Spondyloarthritis (axSpA)
Clinical Features
Inflammatory back pain (IBP) is the hallmark of axSpA. Key features (ASAS criteria): onset <45 years, insidious onset, improvement with exercise, no improvement with rest, and pain at night (with improvement upon getting up).
Diagnosis
Refer to rheumatology. Diagnosis is based on a combination of clinical features, HLA-B27 status, elevated CRP/ESR, and imaging (X-ray sacroiliac joints showing definite sacroiliitis, or MRI showing active inflammation). AxSpA includes radiographic (ankylosing spondylitis) and non-radiographic forms.
Management
First-line: Regular exercise (swimming, Pilates) and NSAIDs (e.g., naproxen, celecoxib). NSAIDs should be taken regularly, not PRN, to control inflammation.
Beyond NSAIDs: Patients with persistently high disease activity are eligible for PBS-subsidised biologic DMARDs (TNF inhibitors like adalimumab, or IL-17 inhibitors like secukinumab) via Authority Required application. Requires rheumatologist initiation.
Allied health: Regular physiotherapy is a cornerstone of management to maintain mobility and posture.
Cauda Equina Red Flags
Red Flag Symptoms & Signs
- Saddle anaesthesia: Altered sensation in the perineum, buttocks, and inner thighs.
- Bladder dysfunction: Urinary retention (overflow incontinence) or loss of bladder sensation.
- Bowel dysfunction: Faecal incontinence or loss of anal sphincter tone.
- Progressive bilateral motor weakness: Especially in the legs (L2-S1 myotomes).
- Sexual dysfunction: Recent onset impotence or altered genital sensation.
Action
If any red flags are present:
- Perform an urgent neurological examination (perianal sensation, anal tone, post-void residual volume).
- Arrange emergency MRI lumbar spine.
- Refer immediately to the nearest neurosurgical or spinal unit.
Imaging Guidelines
Imaging should be guided by clinical assessment and the presence of red flags. Avoid routine imaging for non-specific LBP.
| Indication | First-Line Modality | Notes & MBS Considerations |
|---|---|---|
| Acute LBP, no red flags | No imaging | Reassess if no improvement after 4-6 weeks. |
| Suspected cauda equina, infection, malignancy | MRI (emergency) | Urgent access required. CT myelogram if MRI contraindicated. |
| Progressive neurological deficit | MRI | MBS rebate available with appropriate clinical justification (Item 63001 for MRI lumbar). |
| Suspected axSpA (IBP) | X-ray pelvis (AP) for SI joints | MRI SI joints for non-radiographic disease. Refer rheumatology first. |
| Lumbar stenosis work-up | MRI lumbar spine | Gold standard. CT is alternative if MRI contraindicated. |
| Cervical radiculopathy, persistent | MRI cervical spine | If symptoms persist >6 weeks or with motor deficit. |
Special Populations
LBP/PGP: Common. Use paracetamol as first-line. NSAIDs generally avoided, especially in 3rd trimester. Physiotherapy and pelvic belts are safe.
Imaging: Ultrasound first. MRI (without gadolinium) preferred over CT if needed.
Back pain in children: Uncommon. Always consider serious pathology (tumour, infection, spondylolysis). Pain lasting >4 weeks warrants investigation.
Spondylolysis/Spondylolisthesis: Common in adolescent athletes (gymnastics, cricket). Requires SPECT/CT or MRI for diagnosis.
Osteoporotic Vertebral Fracture: May present with acute LBP after minimal trauma. DXA scan for osteoporosis assessment. Use with caution: NSAIDs (renal/GI risk), opioids (fall risk).
Spinal Stenosis: Prevalence increases with age. Surgical outcomes can be good but must be weighed against comorbidities.
NSAIDs: Avoid if eGFR <30. Use paracetamol. Pregabalin requires dose adjustment.
Paracetamol: Max 2 g/day in severe liver disease. Avoid NSAIDs if cirrhosis. Duloxetine is contraindicated in significant liver disease.
Spinal Infection: Lower threshold for MRI. Presents with localised pain, fever, elevated inflammatory markers. Common organisms: Staph. aureus (including MRSA).
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a higher prevalence of back pain, greater severity, and more significant functional impact. This is compounded by socioeconomic disadvantage, barriers to accessing timely care, and historical distrust of the healthcare system.
📚 References
- 1. Australian Institute of Health and Welfare (AIHW). Back problems. Canberra: AIHW; 2023.
- 2. National Health and Medical Research Council (NHMRC). Australian Acute Musculoskeletal Pain Guidelines. Canberra: NHMRC; 2003 (updated 2020).
- 3. Royal Australian College of General Practitioners (RACGP). Low back pain: clinical care standard. Melbourne: RACGP; 2022.
- 4. Australian Commission on Safety and Quality in Health Care (ACSQHC). Lumbar Spine MRI Clinical Care Standard. Sydney: ACSQHC; 2023.
- 5. Lin I, Wiles L, Waller R, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: systematic review. Br J Sports Med. 2020;54(2):79-86.
- 6. Sieper J, Poddubnyy D. Axial spondyloarthritis. Lancet. 2017;390(10089):73-84.
- 7. Australian Rheumatology Association (ARA). Biological DMARDs for axial spondyloarthritis: information for prescribers. 2024.
- 8. Lurie J, Tomkins-Lane C. Management of lumbar spinal stenosis. BMJ. 2016;352:h6234.
- 9. Medicare Benefits Schedule (MBS) Online. MRI lumbar spine (Item 63001). Australian Government Department of Health. Accessed 2024.
- 10. Painaustralia. National Pain Strategy. 2019.