📋 Key Information Summary
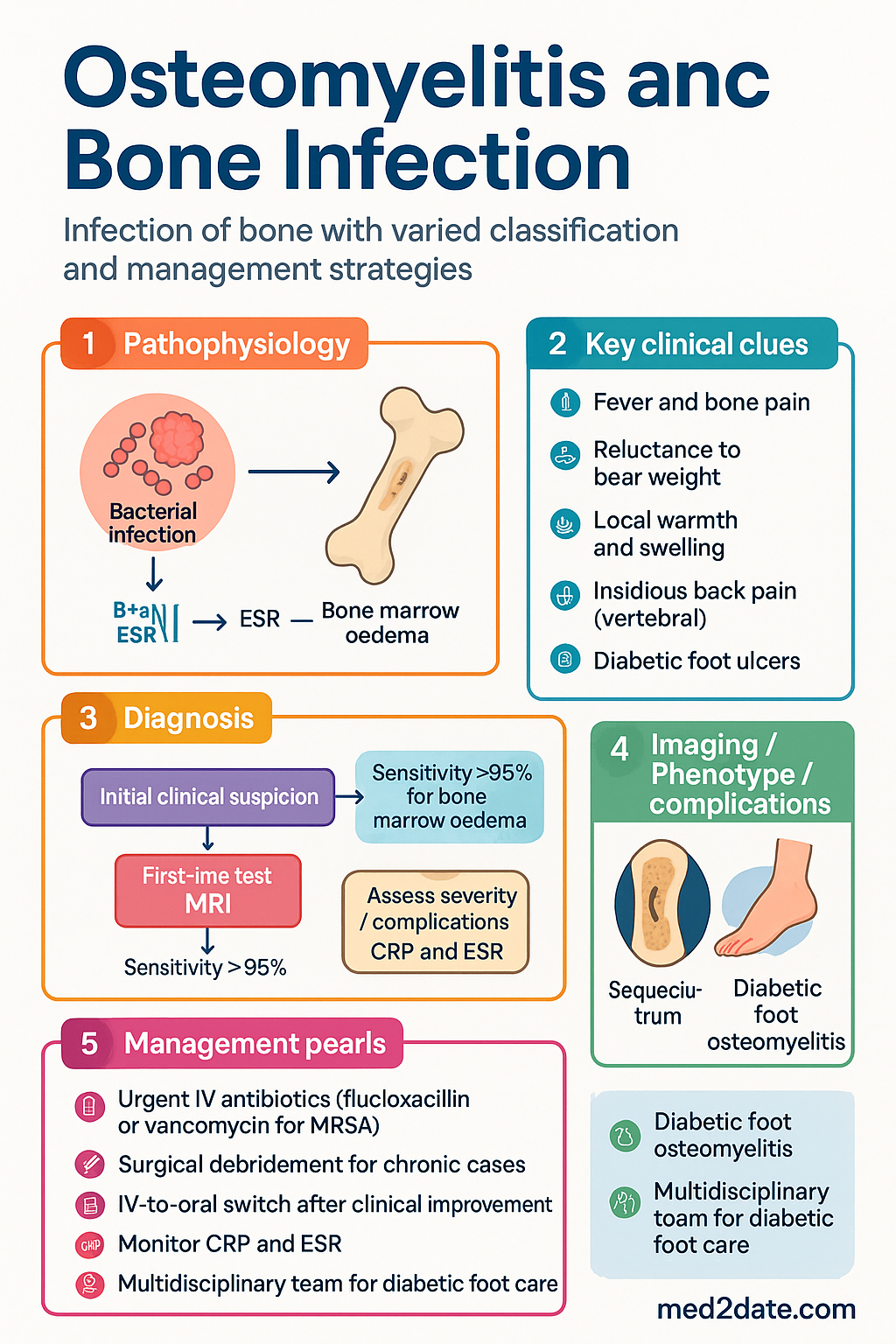
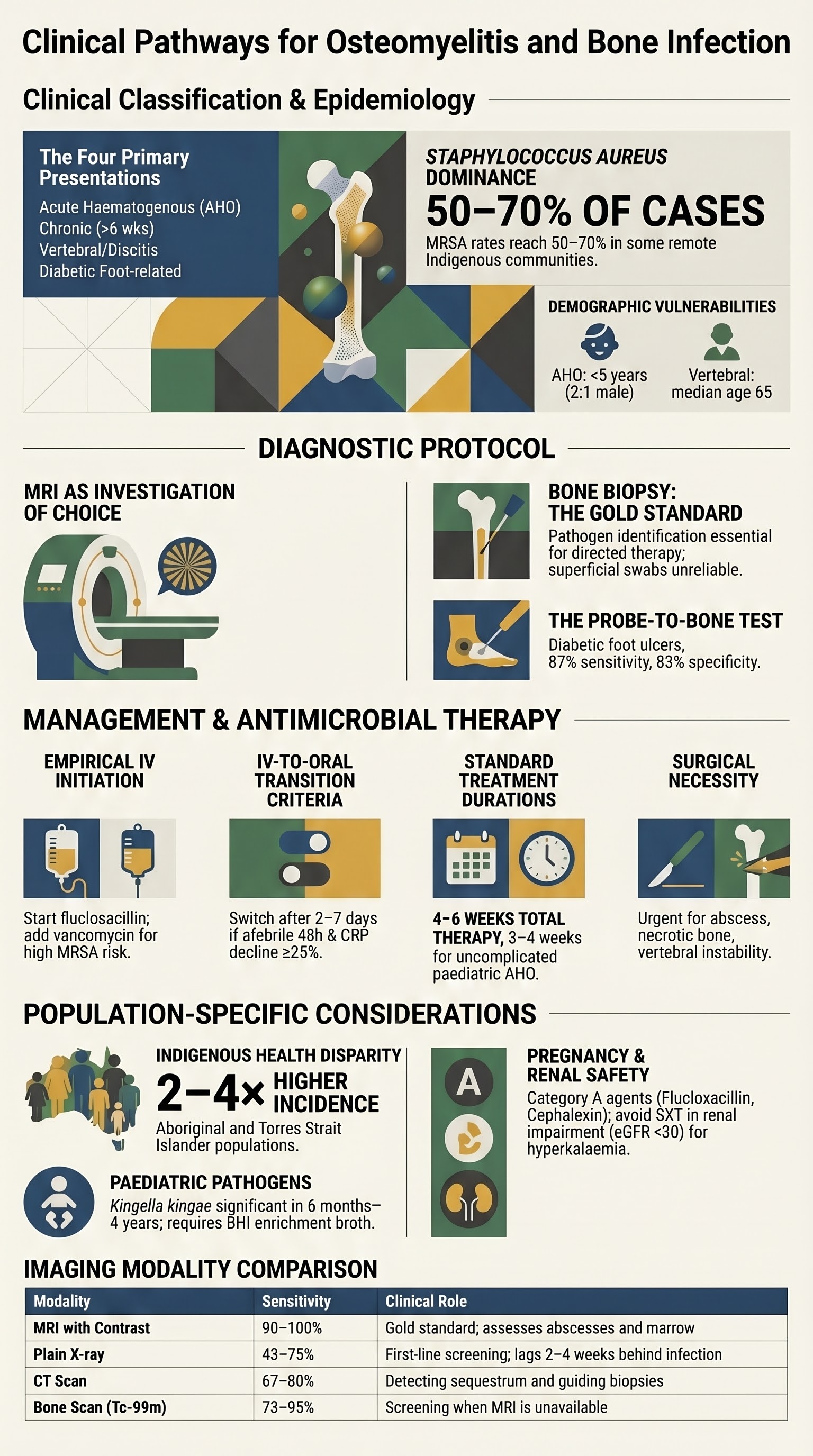
- Osteomyelitis is infection of bone; classification includes acute haematogenous, chronic, vertebral/discitis, and diabetic foot osteomyelitis.
- Staphylococcus aureus (including MRSA) is the most common pathogen across all types; MRSA prevalence varies by Australian region and setting.
- MRI is the investigation of choice for diagnosis; sensitivity >95% for bone marrow oedema. Bone biopsy with culture is the gold standard for pathogen identification.
- Acute haematogenous osteomyelitis: most common in children <5 years. Requires urgent IV antibiotics and surgical drainage if subperiosteal abscess present.
- Chronic osteomyelitis: defined by >6 weeks of symptoms or radiographic sequestrum. Requires surgical debridement combined with prolonged antibiotics.
- Vertebral osteomyelitis: presents with insidious back pain and fever. Most common in lumbar spine. Blood cultures positive in ~60%.
- Diabetic foot osteomyelitis: present in up to 20% of diabetic foot ulcers. Probe-to-bone test has 87% specificity. Can often be managed with oral antibiotics alone if no sepsis.
- Empirical IV therapy: flucloxacillin (or vancomycin if MRSA risk). Directed therapy after culture results. Total duration typically 4–6 weeks (6 weeks for vertebral).
- IV-to-oral switch: possible after 2–7 days of IV therapy if clinical improvement, organism identified, and effective oral agent available (e.g., cephalexin, trimethoprim/sulfamethoxazole).
- CRP and ESR are key monitoring markers; CRP should normalise by 2 weeks. Serial imaging not routinely required.
- Aboriginal and Torres Strait Islander populations have higher osteomyelitis incidence; remote community access and delayed presentation are barriers to optimal care.
- Surgical referral is essential for abscess drainage, debridement, dead-space management, and hardware removal in prosthetic joint infection.
Introduction & Australian Epidemiology
Osteomyelitis is infection of bone caused by bacteria, fungi, or mycobacteria. In Australia, Staphylococcus aureus accounts for approximately 50–70% of cases, with increasing prevalence of community-associated MRSA (CA-MRSA), particularly in northern Australia and remote Indigenous communities.
Key Australian epidemiological points:
- Acute haematogenous osteomyelitis: incidence ~8 per 100,000 in children <5 years; male predominance (2:1).
- Chronic osteomyelitis: rising incidence linked to diabetes, peripheral vascular disease, and prosthetic joint infections.
- Vertebral osteomyelitis: incidence ~2.4 per 100,000; median age 65 years; staphylococci in ~60%.
- Diabetic foot osteomyelitis: affects 10–20% of patients with diabetic foot ulcers during their lifetime.
- CA-MRSA rates in Australia: ~15–20% nationally, up to 50–70% in some remote Indigenous communities.
Acute Haematogenous Osteomyelitis (AHO)
AHO results from bacteraemic seeding of bone. Predominantly affects children, with the metaphysis of long bones (femur, tibia, humerus) most commonly involved.
Risk Factors
- Age <5 years; male sex; recent bacteraemia or soft-tissue infection
- Sickle cell disease (rare in Australia), immunosuppression
- Indwelling IV catheters, trauma, recent surgery
Clinical Features
- Fever, bone pain, reluctance to bear weight/use limb, local warmth and swelling
- Infants may present with pseudoparalysis
- Erythema may be absent early; high clinical suspicion required
Microbiology
| Organism | Frequency | Notes |
|---|---|---|
| S. aureus | 50–70% | Most common; consider CA-MRSA in remote communities |
| Streptococcus spp. | 10–15% | Group A, Group B (neonates), S. pneumoniae |
| Kingella kingae | 5–10% | Children 6 months–4 years; use BHI enrichment broth |
| Gram-negatives | 5% | Neonates (E. coli), sickle cell, immunocompromised |
Initial Management
- IV antibiotics within 1 hour of diagnosis; obtain blood cultures and CRP first.
- Empirical IV: flucloxacillin 50 mg/kg (max 2 g) IV 6-hourly in children; 2 g IV 4–6-hourly in adults.
- If MRSA risk (remote community, prior MRSA): add vancomycin (paediatric 15 mg/kg IV 6-hourly; adult 25–30 mg/kg loading then 15–20 mg/kg IV 12-hourly).
- Consider adding clindamycin 10 mg/kg IV 8-hourly for toxin-mediated strain cover (CA-MRSA).
- IV-to-oral switch after clinical improvement + CRP declining (typically 2–5 days IV).
Oral Step-Down Options
Chronic Osteomyelitis
Defined as osteomyelitis lasting >6 weeks, with sequestrum (dead bone), involucrum, or sinus tract formation. Often polymicrobial. Requires combined surgical and medical therapy.
Classification — Cierny-Mader Staging
Management Principles
- Surgical debridement of necrotic bone and soft tissue is essential — antibiotics alone are insufficient.
- Obtain deep bone/tissue cultures during debridement (not superficial swab).
- Pre-operative IV antibiotics should be withheld until intraoperative cultures obtained (if clinically stable).
- Duration: 6 weeks total (IV + oral) for adequately debrided bone; consider 3–6 months if hardware retained.
- Negative-pressure wound therapy (NPWT) for soft-tissue defects; free-flap coverage may be required.
Vertebral Osteomyelitis & Discitis
Vertebral osteomyelitis accounts for ~2–7% of all osteomyelitis cases. Discitis often co-exists in adults (contiguous spread). The lumbar spine is most commonly affected, followed by thoracic and cervical.
Clinical Features
- Insidious back pain (weeks to months), localised tenderness, low-grade fever (absent in ~30%).
- Neurological deficit in 10–30% (epidural abscess or vertebral collapse).
- ESR and CRP elevated in >90%. Blood cultures positive in ~60%.
Microbiology
| Organism | Frequency | Risk Factors |
|---|---|---|
| S. aureus (incl. MRSA) | 50–60% | IVDU, haemodialysis, prior hospitalisation |
| Gram-negatives | 10–15% | UTI, GU procedures, elderly |
| Mycobacterium tuberculosis | 5–10% | Endemic regions, immunocompromise — consider in all cases |
| Brucella spp. | Rare in Australia | Overseas travel, occupational exposure |
Management
- CT-guided biopsy if blood cultures negative — diagnostic yield ~70%.
- Empirical: flucloxacillin 2 g IV 4–6-hourly + cover gram-negatives if risk factors (add ceftriaxone 2 g IV daily).
- If MRSA: vancomycin 25–30 mg/kg IV loading then 15–20 mg/kg 12-hourly.
- Total duration: 6 weeks minimum (IV 2–4 weeks then oral switch).
- Surgical referral for epidural abscess, progressive neurological deficit, or vertebral instability.
Diabetic Foot Osteomyelitis
Osteomyelitis complicates 10–20% of diabetic foot ulcers. Early diagnosis and appropriate antibiotic duration can avoid amputation in many patients.
Diagnosis
- Probe-to-bone test: sensitivity 87%, specificity 83%. Positive test in the setting of ulcer raises pre-test probability significantly.
- Plain X-ray: low sensitivity early (<50%); may show cortical erosion or periosteal reaction after 2–4 weeks.
- MRI: sensitivity 90%, specificity 80%. Recommended if X-ray equivocal.
- Bone biopsy: gold standard. Perform via cortical window or CT-guided. Yield highest if antibiotic-free for 48 h.
Antibiotic Regimens
Management Approach
- If no systemic sepsis: consider oral antibiotics alone after bone biopsy.
- If soft-tissue infection present: IV antibiotics until soft-tissue infection controlled, then oral switch.
- Duration: 6 weeks if bone infected (shorter courses if bone resected at surgery).
- Offloading and wound care are critical adjuncts; multidisciplinary diabetic foot team referral essential.
MRI & Bone Biopsy
Imaging Strategy
| Modality | Sensitivity | Role | Availability |
|---|---|---|---|
| Plain X-ray | 43–75% | First-line screening; changes lag 2–4 weeks | All centres (MBS) |
| MRI with contrast | 90–100% | Gold standard for diagnosis; assess abscess, sinus tracts | Major/metropolitan centres |
| CT | 67–80% | Sequestrum detection; guided biopsy | Most centres |
| Bone scan (Tc-99m) | 73–95% | Screening when MRI unavailable; limited in diabetic neuropathy | Nuclear medicine centres |
Bone Biopsy — Practical Points
Antibiotic Therapy & Duration
Empirical Therapy — Quick Reference
Directed Therapy by Organism
| Organism | IV Agent | Oral Agent |
|---|---|---|
| MSSA | Flucloxacillin 2 g IV 4–6-hourly | Flucloxacillin 500 mg PO 6-hourly or cephalexin 500 mg PO 6-hourly |
| MRSA (susceptible) | Vancomycin IV (trough 15–20 mg/L) | SXT 160/800 mg PO BD or doxycycline 100 mg PO BD or clindamycin 450 mg PO TDS |
| Streptococcus spp. | Benzylpenicillin 1.2 g IV 6-hourly | Amoxicillin 500 mg PO TDS |
| Gram-negatives | Ceftriaxone 2 g IV daily or meropenem 1 g IV 8-hourly | Ciprofloxacin 500–750 mg PO BD (bone penetration good) |
| Kingella kingae | Ceftriaxone 50 mg/kg IV daily | Amoxicillin 15 mg/kg PO TDS |
IV-to-Oral Switch Criteria
- Afebrile ≥48 hours and improving clinically
- CRP declining (at least 25% fall from peak)
- Organism identified with susceptible oral agent available
- Adequate oral intake and compliance expected
- No evidence of deep abscess requiring further drainage
Monitoring
- CRP: check at baseline, 48–72 h, weekly during treatment. Should normalise by 2 weeks (acute) or show progressive decline.
- ESR: slower to normalise (may remain elevated for months). Less useful for treatment response.
- Vancomycin: monitor trough levels (target 15–20 mg/L for bone infection); adjust for renal function.
- Repeat imaging only if clinical deterioration — early inflammatory changes on MRI may persist for months.
- LFTs if on flucloxacillin >2 weeks; FBC if on SXT or clindamycin.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Kremers HM, Nwojo ME, Ransom JE, et al. Trends in the epidemiology of osteomyelitis: a population-based study, 1969 to 2009. J Bone Joint Surg Am. 2015;97(10):837–845.
- 2. Hatzenbuehler J, Pulling TJ. Diagnosis and management of osteomyelitis. Am Fam Physician. 2011;84(9):1027–1033.
- 3. Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004;364(9431):369–379.
- 4. Li HK, Rombach I, Zambellas R, et al. Oral versus intravenous antibiotics for bone and joint infection (OVIVA). N Engl J Med. 2019;380(5):425–436.
- 5. Spellberg B, Lipsky BA. Systemic antibiotic therapy for chronic osteomyelitis in adults. Clin Infect Dis. 2012;54(3):393–407.
- 6. McNally MA, Nagarajah K. Osteomyelitis. Orthop Trauma. 2018;32(3):175–182.
- 7. Australian Commission on Safety and Quality in Health Care (ACSQHC). Australian Guidelines for the Prevention and Control of Infection in Healthcare. Sydney: ACSQHC; 2019.
- 8. Chihara S, Segreti J. Osteomyelitis. Dis Mon. 2010;56(1):28–45.
- 9. Lipsky BA, Berendt AR, Cornia PB, et al. 2012 IDSA clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2012;54(12):e132–e173.
- 10. Tong SYC, Davis JS, Eichenberger E, et al. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28(3):603–661.
- 11. Berbari EF, Kanj SS, Kowalski TJ, et al. 2015 IDSA clinical practice guideline for the diagnosis and treatment of native vertebral osteomyelitis in adults. Clin Infect Dis. 2015;61(6):e26–e46.
- 12. Australian Indigenous HealthInfoNet. Overview of Aboriginal and Torres Strait Islander health status 2023. Perth: AIHW; 2023.