📋 Key Information Summary
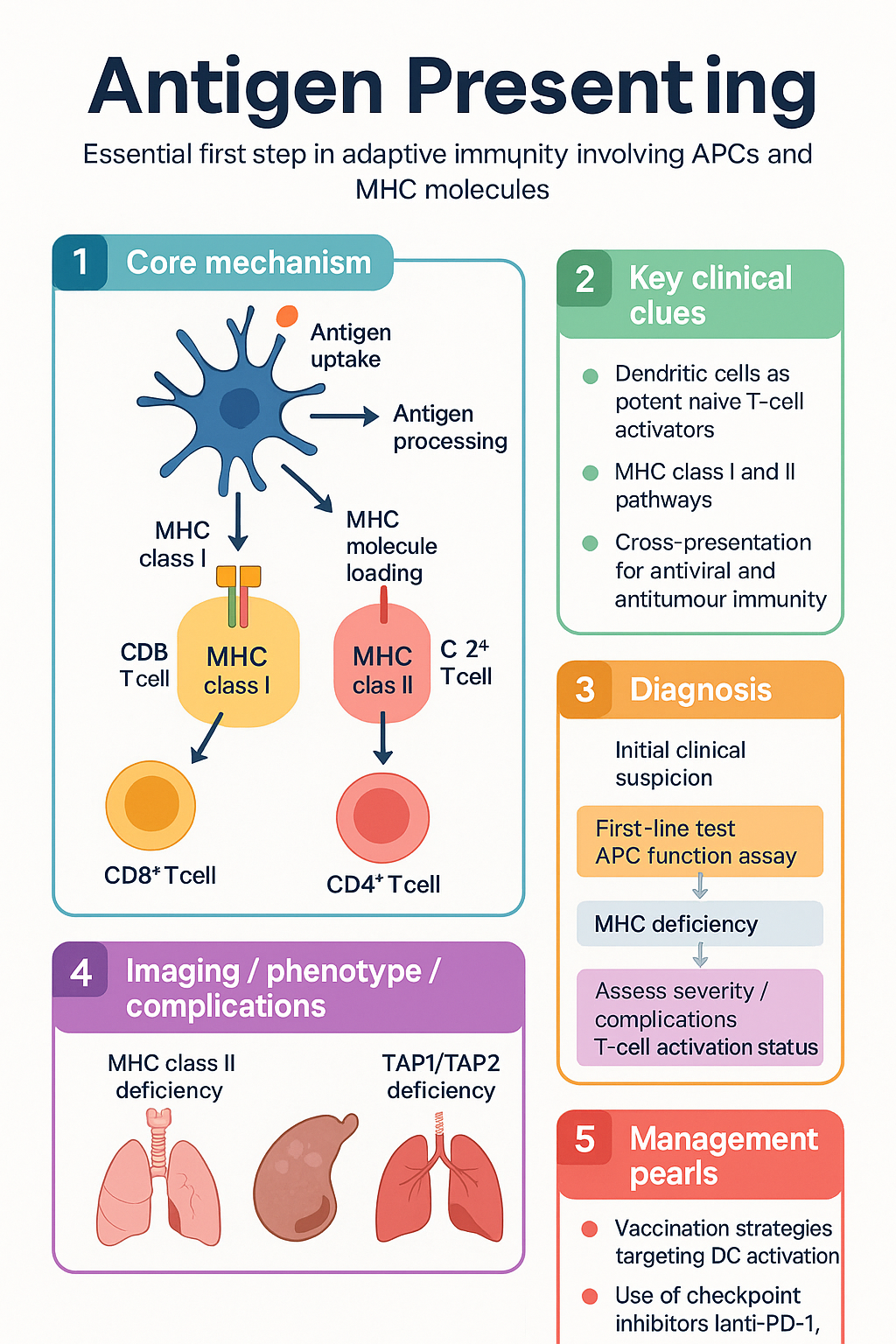
- Antigen-presenting cells (APCs) process protein antigens into peptide fragments and display them on major histocompatibility complex (MHC) molecules for T-cell recognition — the essential first step in adaptive immunity.
- Professional APCs comprise three principal cell types: dendritic cells (DCs), macrophages, and B cells, with DCs being the most potent naïve T-cell activators.
- Two major antigen-processing pathways exist: the MHC class I (endogenous/cytosolic) pathway presents intracellular antigens to CD8⁺ T cells, while the MHC class II (exogenous/endosomal) pathway presents extracellular antigens to CD4⁺ T cells.
- Cross-presentation allows certain DC subsets to load exogenous antigens onto MHC class I molecules, enabling CD8⁺ responses against viruses and tumours that do not directly infect APCs.
- The MHC-peptide-TCR interaction provides two signals for T-cell activation: Signal 1 (antigen-specific) via TCR–pMHC engagement and Signal 2 (co-stimulation) via CD28–B7 or other co-stimulatory pairs.
- Absence of Signal 2 following TCR engagement leads to T-cell anergy — a mechanism of peripheral tolerance exploited therapeutically with CTLA-4-Ig (abatacept).
- Dendritic cell maturation status critically determines immune outcome: immature DCs promote tolerance, while mature DCs promote effector responses.
- Clinical relevance spans vaccination (adjuvant design targets DC activation), transplant immunology (donor APC presentation drives rejection), autoimmune disease (aberrant self-antigen presentation), and immunodeficiency (defective APC function).
- Antigen presentation defects underlie several primary immunodeficiencies, including MHC class II deficiency (bare lymphocyte syndrome type II) and MHC class I deficiency (TAP1/TAP2 deficiency).
- Checkpoint inhibitors (anti-PD-1, anti-CTLA-4) work downstream of antigen presentation to reverse T-cell exhaustion, underscoring the clinical centrality of the APC–T-cell synapse.
Introduction & Australian Context
Antigen-presenting cells (APCs) are specialised immune cells that capture, process, and display peptide fragments on major histocompatibility complex (MHC) molecules to T lymphocytes, thereby initiating and directing adaptive immune responses. This process — antigen presentation — is the central event linking innate pathogen detection to antigen-specific T-cell activation, and it underpins protective immunity, immune tolerance, and immunopathology.
In Australian clinical practice, understanding antigen presentation is directly relevant to vaccination programmes (National Immunisation Programme), transplant medicine, oncology immunotherapy, autoimmune disease management, and the diagnosis of primary immunodeficiencies. Australia's multicultural population and the burden of chronic hepatitis B in Aboriginal and Torres Strait Islander communities highlight the importance of robust APC-mediated CD8⁺ T-cell responses for viral clearance.
This guideline provides a structured overview of professional APCs, antigen-processing pathways, the molecular basis of MHC–peptide–TCR interaction, and the requirements for T-cell activation, with emphasis on clinical applications in the Australian healthcare context.
Professional Antigen-Presenting Cells
Three cell types are classified as professional APCs because they constitutively express MHC class II molecules and provide co-stimulatory signals required for naïve T-cell activation. Non-professional APCs (e.g., epithelial cells, endothelial cells) may upregulate MHC class II under inflammatory conditions but lack the co-stimulatory capacity to prime naïve T cells.
Dendritic Cells
Dendritic cells (DCs) are the most potent professional APCs and are uniquely capable of activating naïve T cells. They are strategically positioned at body surfaces (skin, mucosae) and in lymphoid organs, forming a sentinel network for antigen capture.
| DC Subset | Location | Key Markers | Primary Function |
|---|---|---|---|
| Conventional DC1 (cDC1) | Lymphoid and peripheral tissues | CD141 (BDCA-3), XCR1, CLEC9A | Cross-presentation to CD8⁺ T cells; IL-12 production; antiviral and antitumour immunity |
| Conventional DC2 (cDC2) | Lymphoid and peripheral tissues | CD1c (BDCA-1), CD11b | MHC class II presentation to CD4⁺ T cells; Th1, Th2, Th17 polarisation |
| Plasmacytoid DC (pDC) | Blood, lymphoid tissue | CD303 (BDCA-2), CD123 | Massive type I interferon production; antiviral innate immunity; modest APC function |
| Langerhans cells | Epidermis | CD1a, Langerin (CD207), Birbeck granules | Skin antigen surveillance; capture antigens via extending dendrites |
| Monocyte-derived DC (moDC) | Inflammatory sites | CD14 (variable), CD11c, DC-SIGN | Recruited during inflammation; bridge innate and adaptive immunity |
Macrophages
Macrophages are tissue-resident phagocytes derived from yolk-sac progenitors and circulating monocytes. While primarily effectors of innate immunity (phagocytosis, cytokine production), they serve as important APCs in the context of ongoing infection and inflammation.
- Antigen uptake: Phagocytosis, macropinocytosis, receptor-mediated endocytosis (Fc receptors, complement receptors, mannose receptor)
- MHC class II expression: Constitutive but upregulated by IFN-γ; macrophages are major APCs in granulomatous inflammation (e.g., tuberculosis, sarcoidosis)
- Co-stimulation: Express CD80/CD86 upon activation; less potent than DCs at priming naïve T cells but effective at restimulating effector/memory T cells at sites of inflammation
- Cytokine milieu: M1 macrophages (classically activated) produce IL-12 and promote Th1 responses; M2 macrophages (alternatively activated) produce IL-10 and promote Th2/regulatory responses
- Clinical relevance: In tuberculosis, infected macrophages present mycobacterial antigens to CD4⁺ T cells; granuloma formation depends on macrophage–T-cell interaction. In Australia, TB remains relevant in Aboriginal and Torres Strait Islander communities and among migrants from endemic regions.
B Cells
B lymphocytes function as specialised APCs that capture antigen via their B-cell receptor (BCR/surface immunoglobulin), providing exquisite antigen specificity even at very low antigen concentrations.
- Antigen capture: BCR-mediated endocytosis — the BCR binds native (unprocessed) antigen with high specificity, internalises it, and processes it for MHC class II presentation
- MHC class II expression: Constitutive; upregulated by CD40 ligand (CD154) on activated T cells — the basis of T–B cooperation
- Co-stimulation: Express CD80/CD86 upon activation; also present antigen to CD4⁺ follicular helper T cells (Tfh) in germinal centres
- Functional significance: B-cell antigen presentation to Tfh cells is essential for germinal centre reactions, affinity maturation, class-switch recombination, and long-lived plasma cell/memory B-cell generation
- Clinical relevance: Rituximab (anti-CD20) depletes B cells and reduces B-cell antigen presentation, contributing to its efficacy in B-cell lymphomas and autoimmune diseases (e.g., ANCA-associated vasculitis, rheumatoid arthritis)
Antigen Processing Pathways
Antigen processing refers to the proteolytic degradation of proteins into peptide fragments (typically 8–25 amino acids) that are loaded onto MHC molecules within specific intracellular compartments. The two classical pathways are defined by the source of antigen and the MHC class to which peptides are presented.
MHC Class I Pathway (Endogenous/Cytosolic Pathway)
This pathway processes intracellular proteins — including viral proteins synthesised within infected cells and mutant proteins in tumour cells — for presentation to CD8⁺ cytotoxic T lymphocytes.
MHC Class II Pathway (Exogenous/Endosomal Pathway)
This pathway processes extracellular antigens that have been internalised by professional APCs — via phagocytosis, receptor-mediated endocytosis, or macropinocytosis — for presentation to CD4⁺ T helper cells.
Cross-Presentation
Cross-presentation is a specialised pathway by which certain DC subsets (primarily cDC1) load exogenous antigens onto MHC class I molecules, enabling CD8⁺ cytotoxic T-cell responses against pathogens or tumour cells that do not directly infect APCs.
- Cytosolic pathway: Exogenous antigens escape from endosomes into the cytosol → proteasomal degradation → TAP-dependent ER loading onto MHC class I
- Vacuolar pathway: Antigens are processed by endosomal/lysosomal proteases and loaded onto MHC class I within the endosome itself
- Clinical significance: Cross-presentation is essential for antitumour immunity, antiviral CD8⁺ responses against non-APC-tropic viruses, and the efficacy of many cancer vaccines. Therapeutic strategies to enhance cross-presentation are under active investigation in Australian immunotherapy trials.
MHC-Peptide-TCR Interaction
The physical interaction between the peptide–MHC complex on the APC surface and the T-cell receptor (TCR) on the T lymphocyte is the molecular foundation of adaptive immune recognition. This interaction determines antigen specificity, MHC restriction, and the activation threshold for T-cell responses.
MHC Molecules
| Feature | MHC Class I | MHC Class II |
|---|---|---|
| Gene loci (human) | HLA-A, HLA-B, HLA-C (chromosome 6p21) | HLA-DR, HLA-DQ, HLA-DP (chromosome 6p21) |
| Protein structure | α chain (α1, α2, α3 domains) + β₂-microglobulin | α chain (α1, α2) + β chain (β1, β2) |
| Peptide-binding groove | Closed ends — accommodates 8–11 mer peptides | Open ends — accommodates 13–25+ mer peptides |
| Expression | All nucleated cells; platelets | Professional APCs (constitutive); inducible on others |
| T-cell partner | CD8⁺ cytotoxic T lymphocytes | CD4⁺ T helper cells |
| Accessory molecule | CD8 binds α3 domain — stabilises interaction | CD4 binds β2 domain — stabilises interaction |
TCR Structure and Diversity
- The TCR is a heterodimer of α and β chains (in αβ T cells) or γ and δ chains (in γδ T cells), each comprising variable (V) and constant (C) regions
- TCR diversity is generated by somatic V(D)J recombination during thymic development, yielding an estimated repertoire of >10¹⁵ unique TCRs
- The complementarity-determining region 3 (CDR3) loops of both α and β chains make direct contact with the peptide, providing antigen specificity
- CDR1 and CDR2 loops (germline-encoded) primarily contact the MHC helices, providing MHC restriction
The Immunological Synapse
Upon TCR engagement with pMHC, a specialised junction — the immunological synapse — forms between the T cell and the APC. This supramolecular activation cluster (SMAC) organises signalling molecules for sustained T-cell activation.
- Central SMAC (cSMAC): TCR–pMHC complexes, CD3 signalling complex, co-stimulatory receptors (CD28), PKCθ
- Peripheral SMAC (pSMAC): LFA-1–ICAM-1 adhesion ring — stabilises cell–cell contact
- Distal SMAC (dSMAC): Large phosphatase CD45 — excluded from cSMAC to permit kinase-mediated signalling
TCR Signalling Cascade
TCR engagement triggers a phosphorylation cascade initiated by the Src-family kinase Lck (associated with CD4/CD8 co-receptors):
- Lck phosphorylates ITAMs on CD3ζ chains → recruitment and activation of ZAP-70
- ZAP-70 phosphorylates adaptor proteins LAT and SLP-76 → activation of PLCγ1, Ras-MAPK, and PI3K-Akt pathways
- PLCγ1 cleaves PIP₂ → IP₃ (Ca²⁺ release → NFAT activation) + DAG (PKCθ → NF-κB; RasGRP → AP-1)
- Transcription factors NFAT, NF-κB, and AP-1 cooperatively drive IL-2 production, proliferation, and effector differentiation
HLA Polymorphism and Disease Association
The extreme polymorphism of MHC genes (HLA) in the human population is maintained by balancing selection driven by pathogen diversity. Certain HLA alleles confer disease susceptibility through altered peptide presentation:
| HLA Allele | Associated Disease | Mechanism |
|---|---|---|
| HLA-B27 | Ankylosing spondylitis, reactive arthritis | Presentation of arthritogenic peptides; misfolding triggers UPR/IL-23 |
| HLA-DRB1*04:01/*04:04 | Rheumatoid arthritis | Shared epitope binds citrullinated peptides → anti-CCP antibodies |
| HLA-DQ2/DQ8 | Coeliac disease | Presentation of deamidated gliadin peptides to CD4⁺ T cells |
| HLA-B*57:01 | Abacavir hypersensitivity | Altered peptide repertoire presentation → HLA-restricted drug reaction |
| HLA-B*15:02 | Carbamazepine-induced SJS/TEN | Drug–peptide–HLA complex activates cytotoxic T cells |
T Cell Activation
Full T-cell activation requires the integration of multiple signals delivered at the immunological synapse. The classical two-signal model has been expanded to include a third signal (cytokine polarisation) that determines the effector fate of the activated T cell.
Three-Signal Model of T-Cell Activation
Co-stimulatory and Co-inhibitory Receptors
| T-Cell Receptor | Ligand on APC | Signal Type | Clinical Target |
|---|---|---|---|
| CD28 | CD80 (B7-1), CD86 (B7-2) | Co-stimulatory | Abatacept (CTLA-4-Ig) — blocks CD80/86; used in RA (PBS listed) |
| CTLA-4 | CD80, CD86 (higher affinity) | Co-inhibitory | Ipilimumab (anti-CTLA-4) — checkpoint inhibitor in melanoma (PBS authority) |
| PD-1 | PD-L1 (B7-H1), PD-L2 | Co-inhibitory | Nivolumab, pembrolizumab (anti-PD-1) — melanoma, NSCLC, RCC (PBS listed) |
| ICOS | ICOS-L (B7-H2) | Co-stimulatory | Essential for Tfh function and germinal centre responses |
| LAG-3 | MHC class II | Co-inhibitory | Relatlimab — approved in combination with nivolumab for melanoma |
| TIM-3 | Galectin-9, CEACAM1 | Co-inhibitory | Under investigation in clinical trials for solid tumours |
CD4⁺ T-Helper Cell Subsets
Following activation, CD4⁺ T cells differentiate into functionally distinct subsets determined by Signal 3 cytokines:
| Subset | Master TF | Key Cytokines | Function | Pathology if Dysregulated |
|---|---|---|---|---|
| Th1 | T-bet | IFN-γ, TNF-α, IL-2 | Macrophage activation; intracellular pathogens | Organ-specific autoimmunity (MS, T1DM) |
| Th2 | GATA-3 | IL-4, IL-5, IL-13 | B-cell help; helminth defence | Allergic disease, asthma |
| Th17 | RORγt | IL-17A, IL-17F, IL-22 | Neutrophil recruitment; extracellular bacteria, fungi | Psoriasis, RA, IBD |
| Tfh | Bcl-6 | IL-21, IL-4 | Germinal centre B-cell help; antibody affinity maturation | Autoantibody production; angioimmunoblastic lymphoma |
| Treg | FoxP3 | IL-10, TGF-β, IL-35 | Immune suppression; self-tolerance | IPEX syndrome (loss of FoxP3); reduced antitumour immunity |
CD8⁺ T-Cell Activation and Effector Functions
CD8⁺ cytotoxic T lymphocytes (CTLs) are activated by pMHC class I on any nucleated cell (direct presentation) or on cross-presenting cDC1 (cross-presentation). Full activation requires:
- TCR–pMHC class I engagement (Signal 1)
- CD28 co-stimulation (Signal 2) — typically from the cross-presenting DC
- CD4⁺ T-cell help — CD4⁺ T cells "license" DCs via CD40L–CD40 interaction, upregulating CD80/86 and cytokine production on the DC
CTL effector mechanisms include perforin/granzyme-mediated cytotoxicity (granule exocytosis pathway) and Fas–FasL interaction (death receptor pathway). These mechanisms are central to antiviral immunity and tumour immunosurveillance — and are the basis of checkpoint inhibitor and CAR-T-cell therapy efficacy.
T-Cell Anergy and Peripheral Tolerance
Clinical Applications in Australia
- Vaccination: All National Immunisation Programme vaccines depend on APC-mediated T-cell activation. Adjuvants (AS01, AS04, MF59, aluminium salts) enhance DC maturation and antigen presentation. Live vaccines (MMR, varicella) provide sustained antigen presentation; inactivated vaccines require adjuvants to compensate for lack of endogenous antigen production.
- Checkpoint immunotherapy: Anti-PD-1 (nivolumab, pembrolizumab) and anti-CTLA-4 (ipilimumab) antibodies release the co-inhibitory brake on T cells, restoring effector function against tumour cells. Available via PBS authority for melanoma, NSCLC, RCC, and other indications at Australian cancer centres.
- Transplant immunology: Donor APCs (passenger leucocytes) present alloantigens to recipient T cells (direct allorecognition), while recipient APCs process donor MHC molecules (indirect allorecognition). Both pathways drive acute rejection; immunosuppressive regimens (tacrolimus, mycophenolate, corticosteroids) target T-cell activation downstream of antigen presentation.
- Primary immunodeficiency: MHC class II deficiency (bare lymphocyte syndrome type II, caused by mutations in CIITA, RFXANK, RFX5, or RFXAP) presents in infancy with severe combined immunodeficiency and requires haematopoietic stem cell transplantation — available at Australian paediatric transplant centres (Sydney Children's Hospital, RCH Melbourne).
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Murphy K, Weaver C. Janeway's Immunobiology. 10th ed. New York: Garland Science; 2022.
- 2. Joffre OP, Segura E, Savina A, Amigorena S. Cross-presentation by dendritic cells. Nature Reviews Immunology. 2012;12(8):557–569.
- 3. Banchereau J, Steinman RM. Dendritic cells and the control of immunity. Nature. 1998;392(6673):245–252.
- 4. Neefjes J, Jongsma MLM, Paul P, Bakke O. Towards a systems understanding of MHC class I and MHC class II antigen presentation. Nature Reviews Immunology. 2011;11(12):823–836.
- 5. Smith-Garvin JE, Koretzky GA, Jordan MS. T cell activation. Annual Review of Immunology. 2009;27:591–619.
- 6. Chen L, Flies DB. Molecular mechanisms of T cell co-stimulation and co-inhibition. Nature Reviews Immunology. 2013;13(4):227–242.
- 7. Australian Technical Advisory Group on Immunisation (ATAGI). Australian Immunisation Handbook. Australian Government Department of Health; 2023. Available at: immunisationhandbook.health.gov.au.
- 8. Mallal S, Phillips E, Carosi G, et al. HLA-B*5701 screening for hypersensitivity to abacavir. New England Journal of Medicine. 2008;358(6):568–579.
- 9. Reith W, LeibundGut-Landmann S, Waldburger JM. Regulation of MHC class II gene expression by the class II transactivator. Nature Reviews Immunology. 2005;5(10):793–806.
- 10. Merad M, Sathe P, Helft J, Miller J, Mortha A. The dendritic cell lineage: ontogeny and function of dendritic cells and their subsets in the steady state and the inflamed setting. Annual Review of Immunology. 2013;31:563–604.
- 11. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2023. Canberra: AIHW; 2023.
- 12. Sharpe AH, Pauken KE. The diverse functions of the PD1 inhibitory pathway. Nature Reviews Immunology. 2018;18(3):153–167.