📋 Key Information Summary
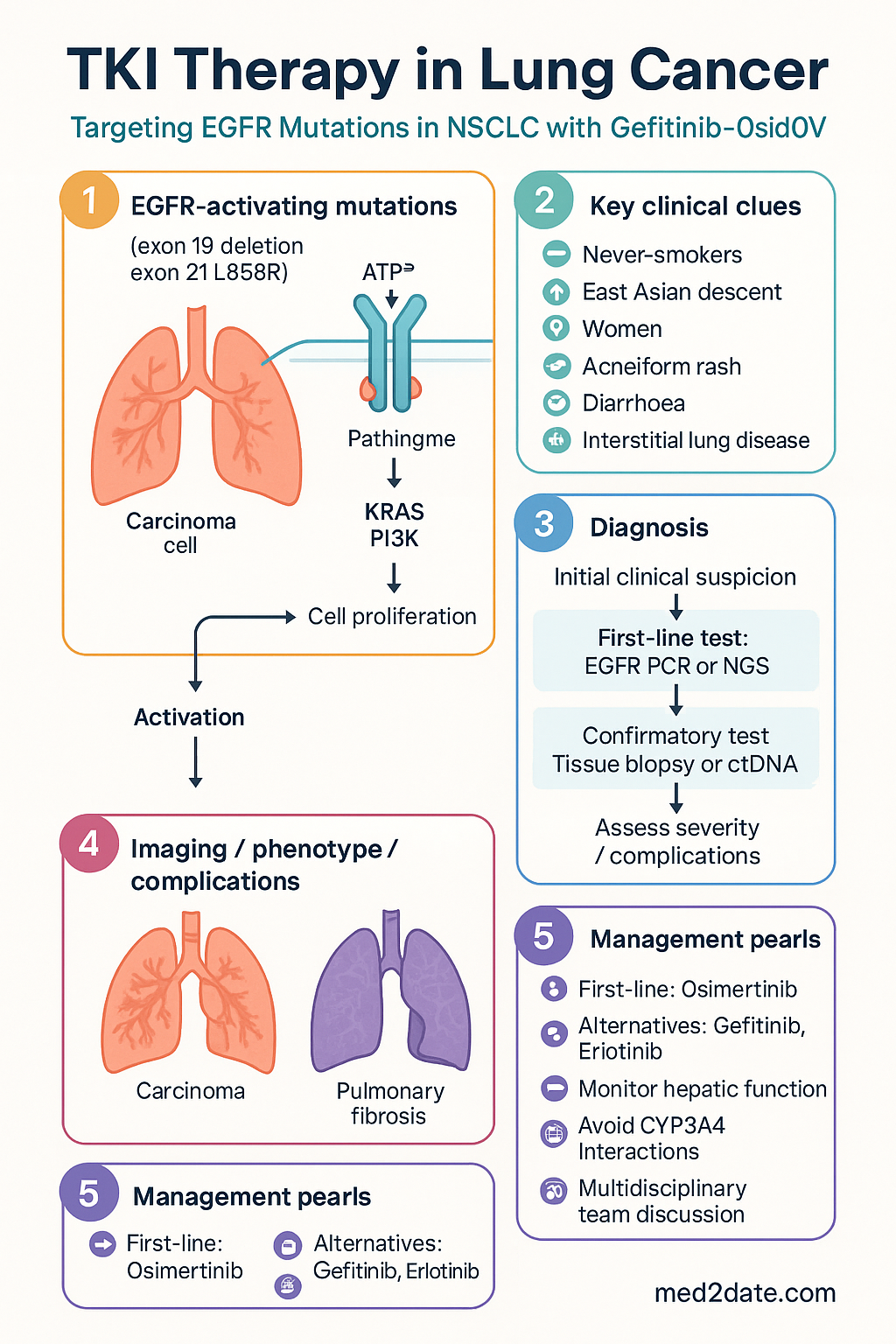
- EGFR-activating mutations (exon 19 deletion, exon 21 L858R) are present in ~10–15% of non-small cell lung cancers (NSCLC) in Australian patients, with higher prevalence in never-smokers, women, and patients of East Asian descent.
- First-line EGFR tyrosine kinase inhibitors (TKIs) — osimertinib, gefitinib, erlotinib — significantly improve progression-free survival (PFS) compared with platinum-based chemotherapy in EGFR-mutant advanced NSCLC.
- Osimertinib (Tagrisso®) is the preferred first-line EGFR TKI in Australia per PBS Authority criteria, offering superior PFS, CNS activity, and a favourable toxicity profile.
- Gefitinib (Iressa®) and erlotinib (Tarceva®) remain PBS-listed first-generation EGFR TKIs; gefitinib is a viable alternative where osimertinib is unavailable or contraindicated.
- Tumour genotyping via next-generation sequencing (NGS) or targeted EGFR PCR is mandatory before initiating any EGFR TKI; tissue biopsy or circulating tumour DNA (ctDNA) testing is available through Australian pathology providers (MBS item 73337).
- The T790M resistance mutation develops in ~50–60% of patients progressing on first- or second-generation EGFR TKIs; osimertinib is the standard second-line therapy for T790M-positive disease.
- Imatinib (Glivec®) is a BCR-ABL and KIT/PDGFRA inhibitor with no primary role in lung cancer; it is the standard of care for chronic myeloid leukaemia (CML) and gastrointestinal stromal tumours (GIST).
- Common adverse effects of EGFR TKIs include acneiform rash (Grade 1–2 in ~70%), diarrhoea, paronychia, and interstitial lung disease (ILD, ~1–3%); hepatic function monitoring is essential.
- Drug interactions: Gefitinib and erlotinib are CYP3A4 substrates — avoid concurrent strong CYP3A4 inducers (e.g., rifampicin) or inhibitors (e.g., itraconazole) without dose adjustment.
- First Nations Australians face lower rates of molecular testing and access to targeted therapies; equitable referral pathways and culturally safe care are essential to closing this gap.
- Multidisciplinary team (MDT) discussion at a recognised cancer centre is mandatory before commencing TKI therapy for any lung cancer patient in Australia.
- All EGFR TKIs listed are PBS Authority Required; prescribers must submit an Authority Prescription with histological and molecular evidence of EGFR-mutant NSCLC.
Introduction & Australian Epidemiology
Tyrosine kinase inhibitors (TKIs) targeting the epidermal growth factor receptor (EGFR) have fundamentally altered the treatment landscape for advanced non-small cell lung cancer (NSCLC). The discovery that somatic activating mutations in the EGFR gene predict dramatic tumour responses to small-molecule EGFR inhibitors ushered in the era of precision oncology in thoracic malignancies.
In Australia, lung cancer remains the fifth most commonly diagnosed cancer and the leading cause of cancer-related mortality, with an estimated 13,810 new cases diagnosed in 2023 and a five-year survival of approximately 22% (Australian Institute of Health and Welfare [AIHW], 2023). NSCLC accounts for ~85% of all lung cancers. Among patients with advanced NSCLC who undergo comprehensive molecular profiling, EGFR-activating mutations are identified in approximately 10–15% of cases — a figure that rises to 40–60% in never-smokers and patients of East Asian ethnicity.
The development and PBS listing of first-generation (gefitinib, erlotinib), second-generation (afatinib), and third-generation (osimertinib) EGFR TKIs in Australia has ensured that patients with EGFR-mutant NSCLC can access targeted oral therapies that offer superior progression-free survival, improved quality of life, and — in the case of osimertinib — a significant overall survival benefit compared with standard platinum-doublet chemotherapy (FLAURA trial; Soria et al., 2018).
Separately, imatinib — a TKI originally developed for BCR-ABL-driven chronic myeloid leukaemia — has no established role in lung cancer. It is discussed here for completeness, given common pharmacological grouping, and to avoid therapeutic confusion. Imatinib's primary indications in Australia remain CML and KIT/PDGFRA-mutant GIST, where it is PBS-listed.
EGFR Biology & Mutations
EGFR Receptor Structure & Signalling
The epidermal growth factor receptor (EGFR, also known as HER1/ErbB1) is a transmembrane receptor tyrosine kinase belonging to the ErbB family. Upon ligand binding (e.g., EGF, TGF-α), EGFR undergoes homo- or heterodimerisation with other ErbB family members, leading to autophosphorylation of intracellular tyrosine residues and activation of downstream signalling cascades, principally:
- RAS–RAF–MEK–ERK (MAPK) pathway: Drives cell proliferation and differentiation.
- PI3K–AKT–mTOR pathway: Promotes cell survival and inhibits apoptosis.
- JAK–STAT pathway: Contributes to transcriptional regulation of survival genes.
- PLCγ–PKC pathway: Modulates calcium signalling and cell motility.
Constitutive activation of EGFR through somatic mutations results in ligand-independent receptor signalling, driving uncontrolled proliferation, angiogenesis, and metastatic potential — the hallmark biology of EGFR-mutant NSCLC.
Clinically Relevant EGFR Mutations
EGFR mutations cluster in the tyrosine kinase domain (exons 18–21). The following are the most clinically significant:
| Mutation | Exon | Frequency (%) | TKI Sensitivity | Clinical Notes |
|---|---|---|---|---|
| Exon 19 deletion (del19) | 19 | ~45% | Highly sensitive | Most common; associated with superior PFS on TKIs vs. L858R |
| L858R point mutation | 21 | ~40% | Sensitive | Second most common; excellent response but shorter PFS than del19 |
| G719X (G719S/C/A) | 18 | ~3% | Sensitive (less common) | Uncommon; response rates lower than del19/L858R |
| S768I | 20 | ~2% | Intermediate sensitivity | Often compound with other EGFR mutations |
| L861Q | 21 | ~2% | Sensitive (less common) | May respond to afatinib or osimertinib |
| Exon 20 insertion | 20 | ~4–10% | Resistant to standard TKIs | Amivantamab + chemo or mobocertinib (limited PBS access) considered |
| T790M (acquired) | 20 | ~50–60% at progression | Resistant to 1st/2nd gen; sensitive to osimertinib | Most common resistance mechanism to gefitinib/erlotinib |
Indications for EGFR Testing in Australia
Molecular testing for EGFR mutations is recommended for all patients with advanced (Stage IIIB/IV) non-squamous NSCLC, and should also be considered in squamous NSCLC in never-smokers or patients with small biopsy specimens where histological subtyping may be uncertain (eviQ / Cancer Institute NSW, 2024). Testing may be performed on:
- Formalin-fixed paraffin-embedded (FFPE) tissue biopsy or cytology specimens
- Circulating tumour DNA (ctDNA) from peripheral blood — useful when tissue is insufficient or unavailable (sensitivity ~70–80%)
- Pleural fluid or other cytology samples with adequate tumour cellularity
Australian pathology laboratories (e.g., Peter MacCallum Cancer Centre, Royal Prince Alfred Hospital, PathWest) perform EGFR testing using validated PCR-based assays or comprehensive next-generation sequencing (NGS) panels. The MBS item 73337 covers genomic profiling for advanced solid tumours.
EGFR Tyrosine Kinase Inhibitors
Three generations of EGFR TKIs are relevant to Australian clinical practice. They differ in mutation selectivity, resistance profiles, CNS penetration, and tolerability.
First-Generation EGFR TKIs
Third-Generation EGFR TKI (Preferred Agent)
Common Adverse Effects of EGFR TKIs
| Adverse Effect | Gefitinib (%) | Erlotinib (%) | Osimertinib (%) | Management |
|---|---|---|---|---|
| Acneiform rash | 66–80% | 75–85% | 45–55% | Doxycycline 100 mg BD prophylaxis; topical clindamycin; Grade 3: dose hold |
| Diarrhoea | 45–55% | 50–60% | 40–50% | Loperamide PRN; hydration; Grade 3: dose hold and rehydrate |
| Paronychia | 15–25% | 20–30% | 25–35% | Silver nitrate, chlorhexidine soaks; avoid tight footwear |
| Dry skin / pruritus | 20–30% | 20–35% | 25–35% | Emollients, soap-free wash; antihistamines |
| Stomatitis | 15–20% | 15–25% | 15–20% | Mouthwash, benzydamine; soft diet |
| Hepatotoxicity (ALT/AST ↑) | 10–15% | 5–10% | 5–8% | LFTs at baseline, fortnightly × 2 months, then monthly |
| Interstitial lung disease (ILD) | 1–3% | 1–2% | ~3–4% | Discontinue immediately; high-dose corticosteroids; exclude infection (BAL) |
| QTc prolongation | Rare | Rare | ~2–5% | Baseline ECG; repeat at 3 weeks; avoid QT-prolonging co-medications |
Imatinib Mechanisms & Indications
Mechanism of Action
Imatinib mesylate (Glivec®) is a small-molecule TKI that competitively binds the ATP-binding site of several tyrosine kinases:
- BCR-ABL: The constitutively active fusion kinase resulting from the Philadelphia chromosome t(9;22) translocation in chronic myeloid leukaemia (CML). Imatinib stabilises the inactive conformation of ABL, blocking downstream RAS/MAPK and JAK/STAT signalling.
- KIT (CD117): A receptor tyrosine kinase mutated or overexpressed in ~80% of gastrointestinal stromal tumours (GIST). Imatinib inhibits constitutive KIT signalling, inducing tumour response and disease control.
- PDGFRA: Platelet-derived growth factor receptor alpha — mutated in a subset of GIST (especially D842V mutation, which confers imatinib resistance).
- CSF-1R, DDR, and other kinases: Additional targets relevant to other indications (e.g., dermatofibrosarcoma protuberans, systemic mastocytosis).
PBS-Approved Indications in Australia
Imatinib was the first TKI to demonstrate that targeted inhibition of a specific oncogenic kinase could produce durable remissions. The IRIS trial (O'Brien et al., NEJM 2003) established imatinib 400 mg as standard first-line therapy for chronic-phase CML, with complete cytogenetic response rates of ~76% and estimated 10-year overall survival of ~83%. In GIST, imatinib achieved disease control in ~80% of patients with advanced disease (Demetri et al., NEJM 2002).
Resistance Mechanisms & Management
Despite the dramatic initial responses to EGFR TKIs, acquired resistance inevitably develops, typically after 9–18 months with first-generation agents and 18–20 months with osimertinib in the first-line setting. Understanding resistance mechanisms guides rational sequencing of subsequent therapies.
Resistance to First-Generation EGFR TKIs (Gefitinib/Erlotinib)
| Mechanism | Frequency | Management Strategy |
|---|---|---|
| EGFR T790M (gatekeeper mutation) | 50–60% | Osimertinib 80 mg daily (PBS-listed for T790M+); rebiopsy or ctDNA at progression |
| MET amplification | 5–20% | Consider combination: osimertinib + MET inhibitor (clinical trial or off-label savolitinib) |
| HER2 amplification | ~13% | Clinical trial enrolment; trastuzumab deruxtecan (T-DXd) in select cases |
| Small cell lung cancer (SCLC) transformation | ~5–15% | Treat as SCLC — platinum/etoposide chemotherapy |
| BRAF V600E mutation | ~1–3% | Dabrafenib + trametinib (off-label consideration) |
| PIK3CA mutation | ~5% | Clinical trial enrolment; limited targeted options currently |
| Unknown / multiple mechanisms | ~20–30% | Chemotherapy ± immunotherapy; clinical trial |
Resistance to Osimertinib (Third-Generation TKI)
Resistance mechanisms to first-line osimertinib are more heterogeneous and less well characterised than those to first-generation TKIs:
- EGFR C797S mutation (~10–15%): The cysteine residue targeted by osimertinib is mutated, abolishing covalent binding. In cis with T790M may respond to combination 1st + 3rd gen TKIs (investigational). In trans configuration may allow gefitinib + osimertinib combination (case reports only).
- MET amplification (~15–20%): Increasingly recognised as a major bypass track. Amivantamab (EGFR/MET bispecific antibody) or savolitinib combinations are under investigation.
- HER2 amplification (~2–10%): Overlap with gefitinib resistance; emerging strategies include T-DXd.
- SCLC transformation (~3–10%): Loss of RB1 and TP53 is characteristic. Treat as SCLC.
- MAPK pathway activation (BRAF, KRAS, NRAS mutations): Diverse and individually rare; clinical trial enrolment recommended.
- Unknown (~30–50%): Represents the largest group; chemotherapy remains standard of care.
Australian Approach to Resistance Workup
Investigations
Risk Stratification & Response Assessment
Response assessment for patients on EGFR TKIs follows RECIST 1.1 criteria with imaging at approximately 8–12 weekly intervals. Prognostic factors influencing outcomes include:
Empirical & Directed Therapy
First-Line Therapy — EGFR-Mutant Advanced NSCLC
Alternative First-Line Agents
- Gefitinib 250 mg PO daily: PBS-listed; suitable if osimertinib unavailable or contraindicated. PFS ~10 months.
- Erlotinib 150 mg PO daily (fasting): PBS-listed; similar efficacy to gefitinib. Higher rates of rash and diarrhoea.
- Afatinib 40 mg PO daily: Second-generation irreversible pan-HER inhibitor; PBS-listed; superior PFS vs. gefitinib in LUX-Lung 7; higher toxicity (diarrhoea, rash). Consider for non-classical EGFR mutations (G719X, L861Q, S768I).
Second-Line Therapy — T790M-Positive Progression
Post-Osimertinib Progression
For patients progressing on first-line osimertinib, the following sequence is generally recommended in Australia:
- Rebiopsy (tissue + ctDNA) to identify resistance mechanism.
- If targetable resistance identified (e.g., MET amplification) — consider clinical trial combination.
- If no targetable resistance — platinum-based doublet chemotherapy (carboplatin AUC 5 + pemetrexed 500 mg/m² Q3W) is standard.
- Add pembrolizumab to chemotherapy only if PD-L1 ≥50% and no contraindication — note increased toxicity of chemo-immunotherapy in EGFR-mutant population (IMpower150 showed benefit with atezolizumab/bevacizumab/carboplatin/paclitaxel in select patients).
- Clinical trial enrolment strongly encouraged (ALTG network).
Adjuvant Therapy — Resected Early-Stage NSCLC
The ADAURA trial (Wu et al., NEJM 2020) demonstrated a disease-free survival benefit with adjuvant osimertinib 80 mg daily for 3 years following complete resection of Stage IB–IIIA EGFR-mutant NSCLC (with or without adjuvant chemotherapy). Osimertinib is PBS-listed for this indication as Authority Required.
Monitoring
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Lung cancer is the most commonly diagnosed cancer and the leading cause of cancer death among Aboriginal and Torres Strait Islander peoples. The age-standardised incidence rate is approximately 1.5 times higher than in the non-Indigenous population, and five-year survival is significantly lower (AIHW, 2023). Disparities in molecular testing rates, access to targeted therapies, and time to treatment initiation are well documented.
📚 References
- 1. Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non–small-cell lung cancer. N Engl J Med. 2018;378(2):113–125. doi:10.1056/NEJMoa1713137
- 2. Mok TS, Wu YL, Ahn MJ, et al. Osimertinib or platinum–pemetrexed in EGFR T790M–positive lung cancer. N Engl J Med. 2017;376(7):629–640. doi:10.1056/NEJMoa1612674
- 3. Wu YL, Tsuboi M, He J, et al. Osimertinib in resected EGFR-mutated non–small-cell lung cancer. N Engl J Med. 2020;383(18):1711–1723. doi:10.1056/NEJMoa2027071
- 4. Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin–paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361(10):947–957. doi:10.1056/NEJMoa0810699
- 5. Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC). Lancet Oncol. 2012;13(3):239–246. doi:10.1016/S1470-2045(11)70393-X
- 6. Park K, Tan EH, O'Byrne K, et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7). Lancet Oncol. 2016;17(5):577–589. doi:10.1016/S1470-2045(16)30033-X
- 7. O'Brien SG, Guilhot F, Larson RA, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2003;348(11):994–1004. doi:10.1056/NEJMoa022457
- 8. Demetri GD, von Mehren M, Blanke CD, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med. 2002;347(7):472–480. doi:10.1056/NEJMoa020461
- 9. Australian Institute of Health and Welfare (AIHW). Cancer data in Australia. Canberra: AIHW; 2023. Available from: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia
- 10. Cancer Institute NSW (eviQ). Non-small cell lung cancer – advanced disease: EGFR mutation positive – gefitinib or erlotinib. eviQ Cancer Treatments Online; 2024. Available from: https://www.eviq.org.au
- 11. National Health and Medical Research Council (NHMRC). Clinical practice guidelines for the prevention, diagnosis and management of lung cancer. Canberra: NHMRC; 2024.
- 12. Australian Government Department of Health. Pharmaceutical Benefits Scheme (PBS). Available from: https://www.pbs.gov.au
- 13. Planchard D, Popat S, Kerr K, et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Suppl 4):iv192–iv237. doi:10.1093/annonc/mdy275
- 14. Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med. 2020;382(1):41–50. doi:10.1056/NEJMoa1913662
- 15. Australian Government Department of Health. National Agreement on Closing the Gap. 2020. Available from: https://www.pmc.gov.au/closing-the-gap