📋 Key Information Summary
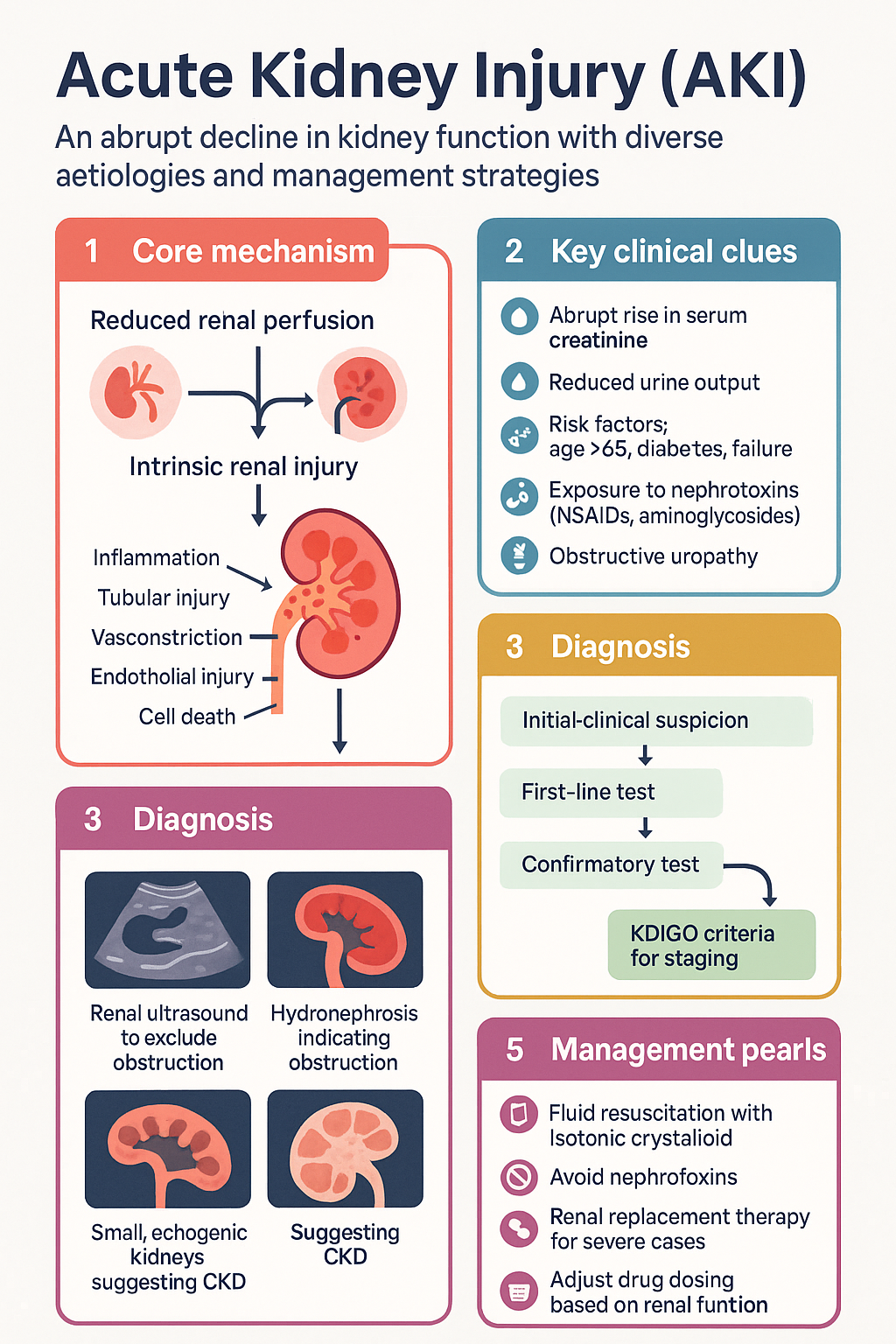
- Definition: Acute kidney injury (AKI) is an abrupt decline in kidney function occurring within hours to days, defined by a rise in serum creatinine (≥26.5 µmol/L within 48 h or ≥1.5× baseline within 7 days) or a fall in urine output (<0.5 mL/kg/h for ≥6 h).
- KDIGO staging (Stage 1–3) guides severity assessment and determines thresholds for renal replacement therapy (RRT).
- Aetiological classification: Pre-renal (55–60 %), intrinsic renal (35–40 %), and post-renal (<5 %) — systematic exclusion of obstruction is mandatory in all cases.
- Urine indices (fractional excretion of sodium, urea, urine osmolality) help differentiate pre-renal azotaemia from intrinsic tubular injury.
- Fluid resuscitation with isotonic crystalloid (0.9 % NaCl or balanced solutions) is first-line for pre-renal AKI; avoid nephrotoxins (NSAIDs, aminoglycosides, iodinated contrast) where possible.
- RRT indications: Refractory hyperkalaemia, severe metabolic acidosis (pH <7.1), pulmonary oedema unresponsive to diuretics, uraemic complications, or specific toxin removal.
- Drug dosing: Renally adjust all renally cleared medications; consult eTG and pharmacy for GFR-based dosing. Aminoglycosides require therapeutic drug monitoring (TDM).
- AKI is preventable: At least 30 % of hospital-acquired AKI is avoidable through early recognition, nephrotoxin avoidance, and haemodynamic optimisation.
- Transition to CKD: AKI episodes increase the risk of chronic kidney disease (CKD) and end-stage kidney disease; post-AKI follow-up with eGFR at 90 days is recommended.
- Aboriginal and Torres Strait Islander peoples have a 2–3× higher incidence of AKI and are more likely to present with advanced disease — culturally safe, community-based pathways improve outcomes.
- Medicare (MBS) items support serum creatinine (item 66500), renal ultrasound (item 55021), and dialysis services in public and private settings.
- Pregnancy-related AKI (pre-eclampsia, HELLP, thrombotic microangiopathy) requires multidisciplinary obstetric–renal management.
Introduction & Australian Epidemiology
Acute kidney injury (AKI) is a common and potentially life-threatening clinical syndrome characterised by an abrupt decline in renal function occurring over hours to days. It encompasses a spectrum from mild, transient elevations in serum creatinine to severe anuric kidney failure requiring renal replacement therapy (RRT). AKI is not a single disease but the final common pathway of diverse insults to the kidney.
In Australia, AKI complicates approximately 15–20 % of all hospital admissions and up to 50 % of intensive care unit (ICU) stays. The Australian Institute of Health and Welfare (AIHW) reports that AKI-related hospitalisations have risen by over 30 % in the past decade, driven by an ageing population, increasing comorbidity burden (diabetes, hypertension, heart failure), and greater use of nephrotoxic agents. In-hospital mortality for AKI ranges from 10 % for Stage 1 to >40 % for Stage 3 requiring dialysis.
Early recognition and timely intervention remain the cornerstones of AKI management. National Safety and Quality Health Service (NSQHS) Standard 9 (Recognising and Responding to Acute Deterioration) mandates the use of early warning scoring systems that incorporate urine output and creatinine trends. The internationally adopted KDIGO (Kidney Disease: Improving Global Outcomes) criteria provide a standardised definition and staging framework, facilitating consistent recognition, research, and audit across Australian hospitals.
KDIGO Classification & Staging
The KDIGO 2012 AKI guideline provides the current standard definition used in Australian practice. AKI is defined by any of the following:
- Increase in serum creatinine ≥26.5 µmol/L (≥0.3 mg/dL) within 48 hours; or
- Increase in serum creatinine to ≥1.5 × baseline, which is known or presumed to have occurred within the prior 7 days; or
- Urine volume <0.5 mL/kg/hour for 6 hours.
| Stage | Serum Creatinine Criteria | Urine Output Criteria |
|---|---|---|
| Stage 1 | 1.5–1.9 × baseline or ≥26.5 µmol/L increase within 48 h | <0.5 mL/kg/h for 6–12 h |
| Stage 2 | 2.0–2.9 × baseline | <0.5 mL/kg/h for ≥12 h |
| Stage 3 | ≥3.0 × baseline or ≥353.6 µmol/L increase or initiation of RRT | <0.3 mL/kg/h for ≥24 h or anuria ≥12 h |
Paediatric modification (pRIFLE): In children, the pRIFLE (paediatric Risk, Injury, Failure, Loss, End-stage) criteria incorporate estimated creatinine clearance (eCCl) and urine output thresholds adjusted for body weight. pRIFLE is more sensitive than KDIGO in detecting AKI in paediatric populations and is recommended by the Australian and New Zealand Paediatric Nephrology Association (ANZPNA).
Risk Factors for AKI in Australian Practice
- Age ≥65 years
- Pre-existing CKD (eGFR <60 mL/min/1.73 m²)
- Diabetes mellitus
- Heart failure or chronic liver disease
- Sepsis or critical illness
- Nephrotoxic drug exposure (NSAIDs, aminoglycosides, iodinated contrast, ACE inhibitors/ARBs in volume depletion)
- Major surgery (especially cardiac, vascular, emergency laparotomy)
- Obstructive uropathy (benign prostatic hyperplasia, urolithiasis)
Pre-renal, Intrinsic & Post-renal Causes
Systematic classification of AKI into pre-renal, intrinsic, and post-renal aetiologies is essential for targeted management. Pre-renal azotaemia accounts for 55–60 % of AKI in hospitalised patients, intrinsic renal injury 35–40 %, and post-renal obstruction <5 %.
- Volume depletion: Haemorrhage, GI losses (vomiting, diarrhoea), burns, third-spacing
- Reduced effective circulating volume: Sepsis, heart failure, cirrhosis, nephrotic syndrome
- Pharmacological: NSAIDs, ACE inhibitors/ARBs, diuretics, calcineurin inhibitors
- Afferent arteriolar constriction: Hepatorenal syndrome, hypercalcaemia
- Acute tubular necrosis (ATN): Ischaemic (prolonged pre-renal), nephrotoxic (aminoglycosides, contrast, cisplatin, myoglobin — rhabdomyolysis)
- Acute interstitial nephritis (AIN): Drug-induced (PPIs, antibiotics — flucloxacillin, NSAIDs), infection-related, autoimmune
- Glomerulonephritis: ANCA-associated vasculitis, anti-GBM disease, lupus nephritis, IgA nephropathy, post-infectious GN
- Vascular: Malignant hypertension, thrombotic microangiopathy (TTP/HUS), renal artery thrombosis/embolism, cholesterol crystal embolisation
- Intratubular obstruction: Uric acid (tumour lysis syndrome), myoglobin, oxalate crystals
- Bladder outflow: Benign prostatic hyperplasia, prostate carcinoma, urethral stricture, neurogenic bladder
- Ureteric: Calculi, malignancy (cervical, bladder, colorectal), retroperitoneal fibrosis, external compression
- Intrarenal: Crystal nephropathy, myeloma cast nephropathy (functional obstruction)
- Bilateral involvement (or unilateral in a solitary kidney) is required to cause AKI
Investigations & Urine Indices
A structured investigation approach should identify the cause, assess severity, and detect complications of AKI.
Baseline Investigations
Urine Indices for Differentiating Pre-renal from Intrinsic AKI
| Index | Pre-renal | Intrinsic (ATN) | Notes |
|---|---|---|---|
| Urine Na⁺ (mmol/L) | <20 | >40 | Unreliable after diuretics |
| FENa (%) | <1 % | >2 % | Invalid if on diuretics; use FEUrea instead |
| FEUrea (%) | <35 % | >50 % | Preferred if patient on diuretics |
| Urine osmolality (mOsm/kg) | >500 | <350 | Kidney's concentrating ability preserved in pre-renal |
| BUN : Creatinine ratio | >100:1 | <40:1 | Reabsorption of urea in pre-renal state |
FENa = (Urine Na × Serum Cr) / (Serum Na × Urine Cr) × 100 %
Fractional excretion of urea (FEUrea) formula:
FEUrea = (Urine Urea × Serum Cr) / (Serum Urea × Urine Cr) × 100 %
Collect a spot urine sample at the same time as bloods. FEUrea is the preferred index in patients already receiving diuretics.
Further Investigations (as Clinically Indicated)
Management & Renal Replacement Therapy
Management of AKI is aetiology-specific but follows universal principles: haemodynamic optimisation, nephrotoxin removal, volume management, metabolic complication control, and timely RRT initiation.
General Supportive Measures
Pharmacological Management
Hyperkalaemia Management — Stepwise Approach
Renal Replacement Therapy (RRT)
RRT should be initiated urgently when life-threatening complications are present, irrespective of a specific creatinine or urea threshold.
Acidosis — refractory metabolic acidosis (pH <7.1 despite bicarbonate)
Electrolytes — refractory hyperkalaemia (K⁺ >6.5 despite medical management)
Intoxication — methanol, ethylene glycol, lithium, salicylates
Overload — fluid overload causing pulmonary oedema unresponsive to diuretics
Uraemia — encephalopathy, pericarditis, bleeding (uraemic platelet dysfunction)
| Modality | Indications | Setting |
|---|---|---|
| Intermittent haemodialysis (IHD) | Haemodynamically stable, rapid clearance needed (hyperkalaemia, intoxication) | Dialysis unit, ward |
| Continuous renal replacement therapy (CRRT) | Haemodynamically unstable (sepsis, vasopressor-dependent), cerebral oedema, acute liver failure | ICU |
| Sustained low-efficiency dialysis (SLED) | Hybrid of IHD and CRRT. Suitable for haemodynamically borderline patients. | ICU, HDU |
| Peritoneal dialysis (PD) | When haemodialysis access unavailable, paediatric AKI, resource-limited settings | Ward, remote/tertiary |
Recovery & Follow-up
- Assess recovery of renal function by serial creatinine measurements. Patients recovering from AKI may undergo a polyuric phase — maintain adequate hydration.
- At 90 days post-AKI, reassess eGFR. Persistent reduction (eGFR <60 mL/min/1.73 m²) defines transition to CKD.
- Refer to nephrology if: eGFR <30, persistent proteinuria, recurrent AKI, or suspected glomerulonephritis.
- Provide patient education: avoid NSAIDs, maintain hydration, monitor weight, attend GP follow-up within 1–2 weeks of discharge.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2(1):1–138.
- 2. STARRT-AKI Investigators; Bagshaw SM, Wald R, Adhikari NKJ, et al. Timing of Initiation of Renal-Replacement Therapy in Acute Kidney Injury. N Engl J Med. 2020;383(3):240–251.
- 3. Barbar SD, Clere-Jehl R, Bourredjem A, et al. Timing of Renal-Replacement Therapy in Patients with Acute Kidney Injury and Sepsis. N Engl J Med. 2018;379(15):1431–1442 (IDEAL-ICU).
- 4. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. Cat. no. PHE 229. Canberra: AIHW; 2023.
- 5. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 6. Kidney Health Australia. Chronic Kidney Disease (CKD) Management in Primary Care. 4th ed. Melbourne: Kidney Health Australia; 2020.
- 7. Hoste EAJ, Kellum JA, Selby NM, et al. Global epidemiology and outcomes of acute kidney injury. Nat Rev Nephrol. 2018;14(10):607–625.
- 8. Hobson CE, Yavas S, Segal MS, et al. Acute kidney injury is associated with increased long-term mortality after cardiothoracic surgery. Circulation. 2009;119(18):2444–2453.
- 9. Mehta RL, Kellum JA, Shah SV, et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31.
- 10. Akcan-Arikan A, Zappitelli M, Loftis LL, et al. Modified RIFLE criteria in critically ill children with acute kidney injury. Kidney Int. 2007;71(10):1028–1035 (pRIFLE criteria).
- 11. Grace BS, Clayton P, McDonald SP. Increases in renal replacement therapy in Australia and New Zealand: understanding trends in diabetic nephropathy. Nephrology. 2012;17(1):76–82.
- 12. Hoy WE, Mott SA, Mc Donald SP. An expanded nationwide view of chronic kidney disease in Aboriginal Australians. Nephrology. 2016;21(11):916–922.
- 13. Lameire NH, Levin A, Kellum JA, et al. Harmonizing acute and chronic kidney disease definition and classification. Kidney Int. 2021;100(3):516–526.