📋 Key Information Summary
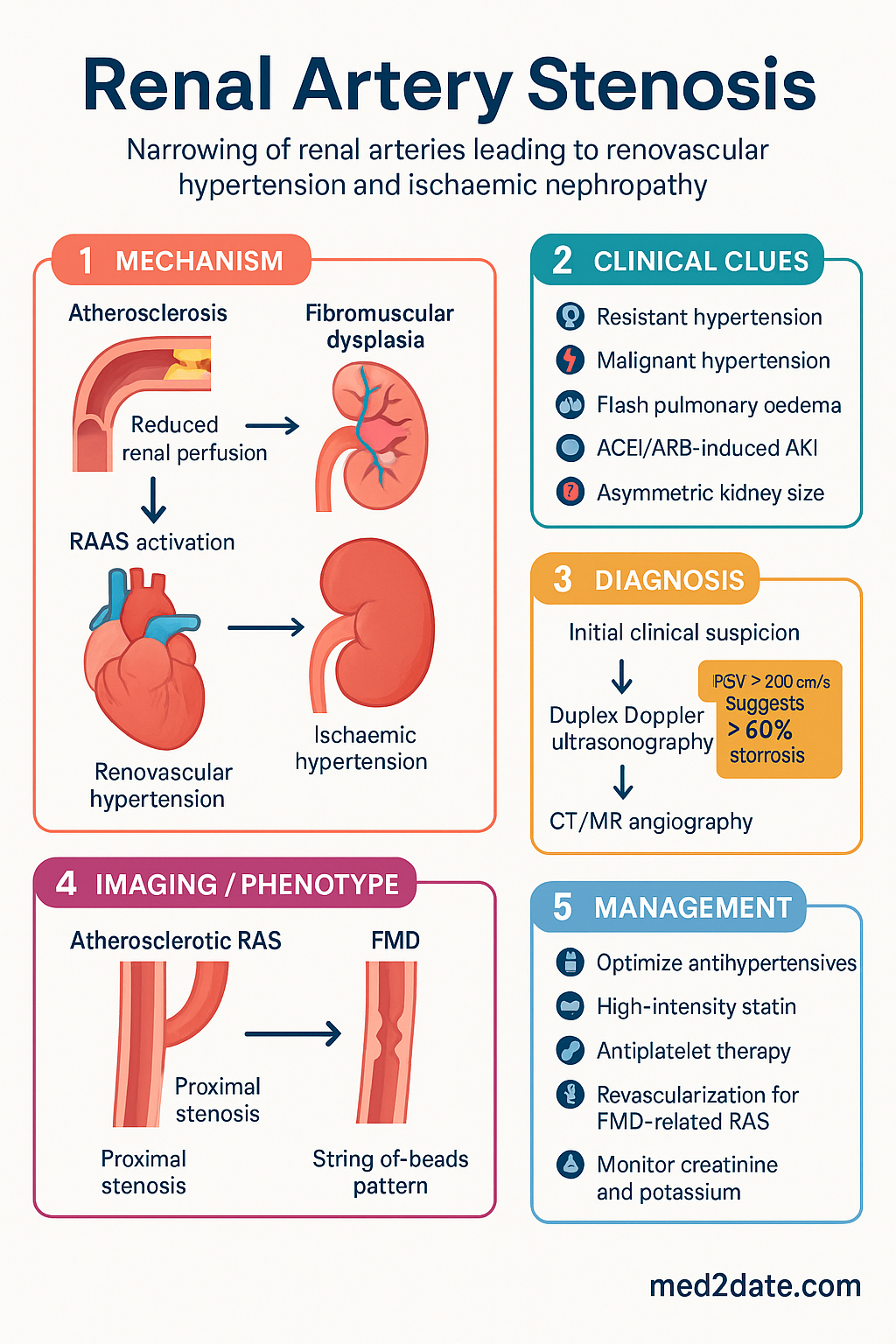
- Renal artery stenosis (RAS) is narrowing of one or both renal arteries, most commonly due to atherosclerosis (~85%) or fibromuscular dysplasia (~10%).
- Atherosclerotic RAS typically affects the ostium and proximal third of the renal artery in patients aged ≥50 with widespread vascular disease (IHD, PVD, CVA).
- Fibromuscular dysplasia (FMD) preferentially affects the mid-to-distal renal artery in young women (<50 years) and may be multifocal or focal.
- Two major consequences: renovascular hypertension (RAAS-mediated) and ischaemic nephropathy (progressive nephron loss from chronic hypoperfusion).
- Suspect RAS in resistant hypertension (requiring ≥3 agents), malignant hypertension, flash pulmonary oedema, unexplained renal function decline after ACE inhibitor/ARB, or asymmetric kidney size ≥1.5 cm difference.
- Duplex Doppler ultrasonography is the preferred first-line screening investigation — non-invasive, widely available, and no contrast required.
- CT angiography or MR angiography confirms diagnosis; conventional catheter angiography remains the gold standard when intervention is planned.
- Medical management is first-line for atherosclerotic RAS: optimise antihypertensives, high-intensity statin, antiplatelet therapy, glycaemic control, and smoking cessation.
- The CORAL and ASTRAL trials demonstrated no significant benefit of renal artery stenting over optimal medical therapy alone in most patients with atherosclerotic RAS.
- Revascularisation (percutaneous transluminal angioplasty ± stenting) is indicated for: FMD-related RAS, flash pulmonary oedema with RAS, progressive renal failure despite medical therapy, and refractory hypertension with ≥70% stenosis.
- Surgical revascularisation (renal endarterectomy or bypass grafting) is reserved for complex anatomy, failed angioplasty, or concurrent aortic surgery.
- ACE inhibitors and ARBs are effective in atherosclerotic RAS but require close monitoring of creatinine and potassium; contraindicated in bilateral RAS or RAS in a solitary functioning kidney.
- Aboriginal and Torres Strait Islander peoples have higher prevalence of CKD and vascular disease — maintain a low threshold for screening RAS in ATSI patients with unexplained hypertension.
Introduction & Australian Epidemiology
Renal artery stenosis (RAS) is the pathological narrowing of the renal artery, leading to reduced renal perfusion, activation of the renin–angiotensin–aldosterone system (RAAS), renovascular hypertension, and progressive ischaemic nephropathy. It remains one of the most common secondary causes of hypertension, though its true prevalence in the general population is debated.
RAS is frequently identified incidentally during angiography performed for other vascular indications. In Australia, RAS is encountered in approximately 5–10% of patients undergoing coronary angiography and up to 30–40% of patients with peripheral vascular disease. Among patients with resistant hypertension defined as uncontrolled blood pressure on three or more antihypertensives (including a diuretic), the prevalence of significant RAS ranges from 10–20%.
The disease burden is increasing in line with Australia's ageing population and the rising prevalence of diabetes, obesity, and dyslipidaemia. Atherosclerotic RAS predominantly affects men aged ≥50 years, while FMD-related RAS is far more common in women aged 15–50 years. Importantly, RAS contributes to 1–5% of all cases of end-stage kidney disease (ESKD) in Australia, and among the over-65 population starting dialysis, renovascular disease accounts for 10–15%.
Aetiology: Atherosclerotic vs Fibromuscular Dysplasia
The two predominant causes of RAS are atherosclerotic disease and fibromuscular dysplasia (FMD). Distinguishing between them is critical, as the prognosis, demographics, and treatment approaches differ significantly.
| Feature | Atherosclerotic RAS | Fibromuscular Dysplasia |
|---|---|---|
| Proportion of all RAS | ~85% | ~10% |
| Demographics | Men ≥50 years | Women 15–50 years |
| Location | Ostium and proximal third | Mid-to-distal artery |
| Angiographic pattern | Focal, irregular plaque | String-of-beads (medial FMD) or focal stenosis |
| Risk factors | Smoking, diabetes, dyslipidaemia, hypertension | Female sex; less linked to traditional CVD risk factors |
| Associated vascular beds | Coronary, carotid, iliac, aortic | Carotid, vertebral, iliac, mesenteric |
| Bilateral | 30–40% | 35–50% |
| Progression | Progressive with plaque growth | Usually stable; aneurysm risk in renal artery |
| Preferred treatment | Medical therapy first; angioplasty if indicated | Percutaneous angioplasty (no stent usually) |
Atherosclerotic Renal Artery Stenosis
Atherosclerotic RAS is a manifestation of systemic atherosclerosis. The stenosis typically involves the aortic ostium or the proximal third of the main renal artery. Risk factors mirror those for other atherosclerotic diseases: advancing age, smoking, hypertension, dyslipidaemia, diabetes mellitus, and chronic kidney disease. There is a strong association with coronary artery disease, peripheral vascular disease, and carotid stenosis. The disease tends to be progressive — approximately 50% of lesions with >60% stenosis at baseline will progress over 3–5 years if untreated.
Fibromuscular Dysplasia
FMD is a non-atherosclerotic, non-inflammatory arterial disease. The 2019 consensus statement classifies FMD into multifocal (the classic string-of-beads appearance, predominantly medial fibroplasia) and focal subtypes. Multifocal FMD accounts for approximately 80–90% of cases and is the more common form in the renal arteries. Focal FMD is less common but may present at a younger age and is more frequently associated with hypertension. FMD can involve multiple vascular beds, and up to two-thirds of patients with renal FMD have extrarenal involvement — most commonly carotid and vertebral arteries.
Other Causes (Rare)
- Takayasu arteritis — large-vessel vasculitis affecting the aorta and its branches; more common in young Asian women.
- Arterial dissection — spontaneous or traumatic.
- Neurofibromatosis type 1 — vascular stenosis from intimal proliferation.
- Radiation-induced arteriopathy — following abdominal or retroperitoneal radiotherapy.
- Renal artery aneurysm with secondary stenosis.
- Extrinsic compression — from tumours or retroperitoneal fibrosis.
Clinical Features & Presentation
Many patients with RAS are asymptomatic, and the condition is frequently discovered incidentally during imaging for other vascular pathology. When symptoms occur, they are related to the two major consequences of renal artery narrowing: renovascular hypertension and ischaemic nephropathy.
Presenting Features Suggestive of RAS
| Clinical Clue | Details |
|---|---|
| Resistant hypertension | Uncontrolled BP despite ≥3 antihypertensives (including a diuretic at adequate dose) |
| Malignant/accelerated hypertension | BP >180/120 mmHg with papilloedema, haematuria, or renal impairment |
| New-onset hypertension <30 or >55 years | Atypical age for primary hypertension; particularly young women (FMD) |
| Flash pulmonary oedema | Acute pulmonary oedema with normal LV function; strongly suggests bilateral RAS |
| ACEi/ARB-induced AKI | Rise in serum creatinine ≥30% within 1–2 weeks of starting RAAS blockade |
| Asymmetric kidney size | Difference in renal length ≥1.5 cm on ultrasound |
| Unexplained renal impairment | Progressive CKD without clear parenchymal cause; small, shrunken kidneys |
| Abdominal/renal bruit | Systolic-diastolic bruit in the epigastrium or flank; specificity high but sensitivity low (~40%) |
| Widespread atherosclerosis | Patients with known coronary, peripheral vascular, or cerebrovascular disease |
| Recurrent pulmonary oedema with renal failure | Combined cardiorenal syndrome picture |
Presentation Patterns by Aetiology
Pathophysiology
Understanding the pathophysiology of RAS is essential for rational management. Renal artery narrowing triggers a cascade of haemodynamic and neurohormonal responses that perpetuate both hypertension and renal injury.
The Two-Kidney, One-Clip Model
In unilateral RAS (the classic Goldblatt model), the stenosed kidney experiences reduced perfusion pressure. This leads to:
- Juxtaglomerular apparatus activation: Renal ischaemia stimulates renin release from juxtaglomerular cells.
- Angiotensin II elevation: Renin cleaves angiotensinogen to angiotensin I; ACE converts it to angiotensin II, causing systemic vasoconstriction and aldosterone secretion.
- Sodium retention: Aldosterone promotes sodium reabsorption in the distal nephron, expanding plasma volume.
- Systemic hypertension: The combination of vasoconstriction and volume expansion raises blood pressure, which the contralateral (non-stenosed) kidney must excrete. This is termed "renin-dependent" or "renovascular" hypertension.
The One-Kidney, One-Clip Model
In bilateral RAS or RAS in a solitary functioning kidney, both kidneys (or the only kidney) are underperfused. Sodium excretion is impaired because there is no "escape" kidney. Hypertension in this setting is primarily volume-dependent rather than renin-dependent, and RAAS blockade may precipitate AKI because the kidney relies on angiotensin II–mediated efferent arteriolar constriction to maintain glomerular filtration pressure.
Ischaemic Nephropathy
Chronic reduction in renal blood flow leads to tubular atrophy, interstitial fibrosis, and glomerulosclerosis. The tubulointerstitial changes are the hallmark of ischaemic nephropathy and may be irreversible even after successful revascularisation, explaining why revascularisation does not always restore renal function.
Investigations
Investigation of suspected RAS involves screening tests, confirmatory imaging, and functional assessment. Selection depends on clinical context, renal function, and local availability.
Screening & Confirmatory Investigations
Baseline Investigations
- Serum creatinine and eGFR — assess baseline renal function and detect asymmetry.
- Serum electrolytes — hypokalaemia may suggest hyperaldosteronism secondary to RAAS activation.
- Plasma renin activity (PRA) and aldosterone — may be elevated in unilateral RAS (high renin hypertension).
- Urinalysis — proteinuria, haematuria, casts to exclude parenchymal renal disease.
- Full blood count — assess for secondary erythrocytosis (from elevated erythropoietin) or anaemia of CKD.
- Lipid profile and HbA1c — assess cardiovascular risk factors that require optimisation.
- Renal length on ultrasound — asymmetry of ≥1.5 cm suggests chronic ischaemia on the smaller side.
Risk Stratification & Severity
Risk stratification guides the decision between conservative medical management and interventional revascularisation. The degree of stenosis alone is insufficient — clinical context, renal function trajectory, and blood pressure control must all be considered.
Predictors of Poor Response to Revascularisation
- Resistive index (RI) >0.80 on Doppler ultrasound — suggests irreversible parenchymal damage.
- Kidney length <7 cm — severely atrophied kidneys unlikely to recover function.
- Long-standing renal impairment (>6 months of high creatinine).
- Heavy proteinuria (>1 g/day) — may indicate coexisting parenchymal disease.
- Diffuse small-vessel disease on angiography.
Management
Management of RAS requires a multidisciplinary approach involving nephrology, vascular surgery, interventional radiology, and the patient's general practitioner. The optimal strategy depends on aetiology, clinical severity, and comorbidities.
Medical Management (First-Line for Atherosclerotic RAS)
Following the landmark ASTRAL (2009) and CORAL (2014) randomised controlled trials, optimal medical therapy has become the cornerstone of management for most patients with atherosclerotic RAS. Neither trial demonstrated a significant benefit of renal artery stenting over medical therapy alone for the composite outcomes of cardiovascular events, renal events, or death.
Interventional Management
Indications for Revascularisation
- FMD-related RAS (angioplasty is first-line therapy)
- Recurrent flash pulmonary oedema with significant (≥70%) RAS
- Progressive renal impairment attributed to RAS despite optimal medical therapy
- Malignant or refractory hypertension with ≥70% stenosis and failure of ≥3 antihypertensive agents
- RAS in a solitary functioning kidney with declining function
- Bilateral RAS with progressive CKD
Post-Intervention Monitoring
- Serum creatinine and potassium at 1, 3, and 7 days post-procedure, then monthly for 3 months.
- Blood pressure monitoring — expect reduction in first 1–2 weeks if intervention was successful.
- Duplex Doppler ultrasound at 1 month, 6 months, and then annually to detect restenosis (which occurs in 10–20% of atherosclerotic cases within 2 years).
- Continue dual antiplatelet therapy (aspirin + clopidogrel) for 4–6 weeks post-stenting, then aspirin indefinitely.
- Maintain high-intensity statin therapy and cardiovascular risk factor modification lifelong.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Cooper CJ, Murphy TP, Cutlip DE, et al. Stenting and medical therapy for atherosclerotic renal-artery stenosis. N Engl J Med. 2014;370(1):13–22. doi:10.1056/NEJMoa1310753
- 2. ASTRAL Investigators; Wheatley K, Ives N, Gray R, et al. Revascularization versus medical therapy for renal-artery stenosis. N Engl J Med. 2009;361(20):1953–1962. doi:10.1056/NEJMoa0905368
- 3. Gornik HL, Persu A, Adlam D, et al. First international consensus on the diagnosis and management of fibromuscular dysplasia. Vasc Med. 2019;24(2):164–189. doi:10.1177/1358863X18821816
- 4. Textor SC. Renovascular hypertension and ischaemic nephropathy. In: Skorecki K, Chertow GM, Marsden PA, et al., eds. Brenner and Rector's The Kidney. 11th ed. Philadelphia: Elsevier; 2020:1267–1297.
- 5. Rundback JH, Sacks D, Kent KC, et al. Guidelines for the reporting of renal artery revascularization in clinical trials. J Vasc Interv Radiol. 2003;14(9 Pt 2):S477–S492.
- 6. National Heart Foundation of Australia. Guideline for the diagnosis and management of hypertension in adults. Melbourne: National Heart Foundation of Australia; 2016.
- 7. Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO 2021 clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 2021;99(3):S1–S87.
- 8. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. Cat. no. PHE 224. Canberra: AIHW; 2023.
- 9. Rossi GP, Seccia TM, Barton M, et al. Endovascular revascularization for atherosclerotic renal artery stenosis: the Endovascular versus open surgical revascularization (EROR) study. Eur Heart J. 2021;42(38):3920–3930. doi:10.1093/eurheartj/ehab469
- 10. Olin JW, Gornik HL, Bacharach JM, et al. Fibromuscular dysplasia: state of the science and critical unanswered questions. Circulation. 2014;129(18):1866–1878. doi:10.1161/CIRCULATIONAHA.113.002620
- 11. Ritchie A, Hockley B, Dwyer KM. Renovascular disease in Aboriginal and Torres Strait Islander Australians. Nephrology. 2020;25(6):439–445. doi:10.1111/nep.13722
- 12. Khosla S, White CJ, Collins TJ, et al. Effects of renal artery stent implantation in patients with renovascular hypertension presenting with unstable angina or congestive heart failure. Am J Cardiol. 1997;80(3):363–366.