📋 Key Information Summary
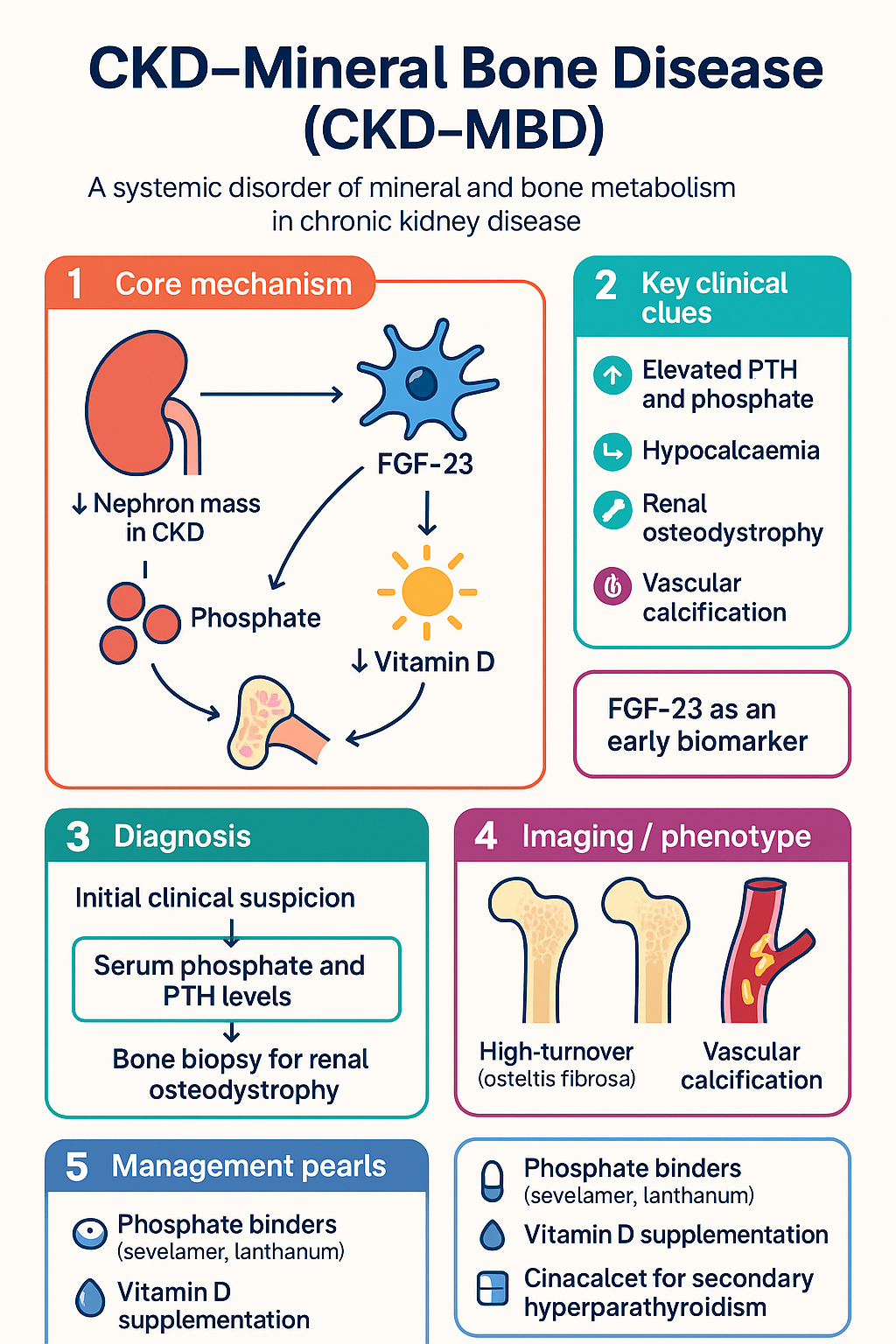
- CKD-MBD is a systemic disorder encompassing biochemical abnormalities (elevated PTH, hyperphosphataemia, hypocalcaemia, raised FGF-23), bone abnormalities (renal osteodystrophy), and vascular/soft-tissue calcification.
- FGF-23 is the earliest biomarker to rise (CKD 2–3), preceding phosphate and PTH elevations by months to years.
- Phosphate targets: serum phosphate maintained within the age-appropriate reference range; target 0.8–1.5 mmol/L in adults on dialysis.
- PTH targets in dialysis: 2–9× the upper limit of normal for intact PTH assay; trends matter more than individual values.
- Corrected calcium should be maintained within the normal reference range (2.10–2.55 mmol/L); avoid hypercalcaemia and adynamic bone disease.
- Renal osteodystrophy has two major subtypes: high-turnover (osteitis fibrosa, secondary hyperparathyroidism) and low-turnover (adynamic bone disease, osteomalacia).
- Phosphate binders are first-line for hyperphosphataemia: sevelamer or lanthanum preferred over calcium-based binders to reduce vascular calcification risk.
- Calcitriol (1,25-dihydroxyvitamin D) or alfacalcidol is used to suppress secondary hyperparathyroidism; native vitamin D (cholecalciferol) should be supplemented in all CKD patients with insufficiency.
- Cinacalcet is PBS Authority Required for dialysis patients with secondary hyperparathyroidism uncontrolled despite phosphate binders and vitamin D therapy.
- Vascular calcification screening (lateral abdominal X-ray or CT) should be considered in CKD 4–5 as it independently predicts cardiovascular mortality.
- Aboriginal and Torres Strait Islander peoples have higher CKD prevalence, younger age at dialysis commencement, and reduced access to specialist nephrology services — CKD-MBD screening must begin earlier.
- Parathyroidectomy is reserved for refractory tertiary hyperparathyroidism or severe symptomatic disease; subtotal or total with auto-transplant is standard.
Introduction & Australian Epidemiology
Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD) is a systemic disorder of mineral and bone metabolism that occurs in progressive chronic kidney disease. It encompasses three interrelated components: biochemical abnormalities (elevated PTH, hyperphosphataemia, hypocalcaemia, and raised FGF-23), bone abnormalities collectively termed renal osteodystrophy, and vascular or soft-tissue calcification. CKD-MBD is a major driver of morbidity and mortality in patients with CKD stages 3–5 and those receiving dialysis, primarily through accelerated cardiovascular disease and fracture risk.
In Australia, CKD-MBD affects the majority of patients on maintenance dialysis. Data from the Australia and New Zealand Dialysis and Transplant (ANZDATA) Registry indicate that approximately 50–60% of prevalent haemodialysis patients have elevated serum phosphate, and over 80% exhibit elevated intact PTH levels. Vascular calcification is detectable in up to 80% of patients commencing dialysis. The disease burden is disproportionately borne by Aboriginal and Torres Strait Islander peoples, who develop end-stage kidney disease at rates 6–8 times higher than non-Indigenous Australians and often present with more severe mineral bone disease at younger ages.
The economic burden of CKD-MBD is significant. Phosphate binders, active vitamin D analogues, and calcimimetics represent substantial pharmaceutical expenditure through the Pharmaceutical Benefits Scheme (PBS), while vascular calcification-related cardiovascular events contribute to hospitalisation costs estimated at over .5 billion annually for CKD care in Australia.
Pathophysiology — FGF-23, PTH, and Vitamin D
The pathophysiology of CKD-MBD involves a cascade of endocrine and paracrine disturbances that begin early in CKD and progress with declining nephron mass. Three key hormonal axes are central: fibroblast growth factor 23 (FGF-23), parathyroid hormone (PTH), and the vitamin D axis.
FGF-23 — The Earliest Abnormality
FGF-23, a phosphaturic hormone secreted by osteocytes, is the earliest detectable abnormality in CKD-MBD, rising from CKD stage 2–3 — well before serum phosphate becomes elevated. FGF-23 acts on the proximal tubule to promote urinary phosphate excretion and suppresses 1α-hydroxylase activity, reducing calcitriol (1,25-dihydroxyvitamin D) production. As nephron mass declines, the compensatory rise in FGF-23 becomes insufficient to maintain phosphate homeostasis, leading to positive phosphate balance and subsequent PTH elevation.
Elevated FGF-23 is independently associated with left ventricular hypertrophy, cardiovascular events, and all-cause mortality in CKD. It is not yet routinely measured in Australian clinical practice but is an important biomarker in research and increasingly in specialist nephrology assessment.
Parathyroid Hormone (PTH) — Secondary Hyperparathyroidism
Secondary hyperparathyroidism develops through several mechanisms:
- Phosphate retention: Directly stimulates PTH secretion and reduces ionised calcium.
- Calcitriol deficiency: Reduced vitamin D receptor (VDR) activation on parathyroid glands decreases PTH gene suppression and reduces intestinal calcium absorption.
- Hypocalcaemia: Stimulates PTH release via the calcium-sensing receptor (CaSR) on chief cells.
- FGF-23 effects: FGF-23 directly acts on parathyroid glands to suppress PTH secretion (via FGFR/Klotho), but parathyroid resistance develops over time.
- Parathyroid gland hyperplasia: Chronic stimulation leads to nodular hyperplasia, eventually causing autonomous (tertiary) hyperparathyroidism with reduced response to medical therapy.
PTH acts on bone to increase osteoblast activity and bone turnover. Chronically elevated PTH leads to high-turnover bone disease (osteitis fibrosa cystica), cortical bone loss, and fracture risk. PTH also contributes to vascular calcification indirectly through increased bone resorption and calcium/phosphate release.
Vitamin D Axis
Two vitamin D derangements occur in CKD:
- Native vitamin D (25-hydroxyvitamin D) deficiency: Present in 60–80% of CKD patients due to reduced sun exposure, proteinuria (vitamin D binding protein loss), reduced skin synthesis, and dietary restriction. Cholecalciferol supplementation is recommended for all CKD patients with levels <75 nmol/L.
- Calcitriol (1,25-dihydroxyvitamin D) deficiency: Results from reduced 1α-hydroxylase activity in the failing kidney and FGF-23-mediated suppression. This is the key driver of secondary hyperparathyroidism and is treated with active vitamin D analogues (calcitriol or alfacalcidol).
The interplay of these three axes creates a vicious cycle: FGF-23 rises → calcitriol falls → PTH rises → phosphate remains elevated → parathyroid hyperplasia → autonomous secretion. Breaking this cycle at multiple points is the therapeutic goal.
Vascular Calcification
CKD-MBD promotes vascular calcification through both passive (metastatic) deposition of calcium-phosphate in the media and intima, and active processes including transformation of vascular smooth muscle cells to an osteoblast-like phenotype. Elevated calcium × phosphate product, hyperphosphataemia, and calcium overload from calcium-based phosphate binders are key drivers. Calcification inhibitors — fetuin-A, matrix Gla protein, and pyrophosphate — are reduced in CKD. Medial calcification increases arterial stiffness and pulse pressure, contributing to the disproportionately high cardiovascular mortality in CKD.
Renal Osteodystrophy Types
Renal osteodystrophy (ROD) is the bone component of CKD-MBD. Histological classification requires bone biopsy (gold standard), though in practice, biochemical markers and imaging are used for diagnosis. The Kidney Disease: Improving Global Outcomes (KDIGO) classification uses the TMV system (Turnover, Mineralisation, Volume).
Fracture Risk in CKD-MBD
Fracture rates in CKD stages 4–5 and dialysis patients are 2–4 times higher than age-matched populations. Hip fractures carry a 1-year mortality of 30–40% in dialysis patients. Both high-turnover and low-turnover disease increase fracture risk through different mechanisms: cortical porosity (osteitis fibrosa) and reduced bone formation (ABD). Standard DXA BMD has limited predictive value in CKD 5D due to concurrent cortical and trabecular abnormalities and vascular calcification artefact.
Investigations & Targets
Biochemical monitoring of CKD-MBD should commence from CKD stage 3 and be performed at increasing frequency with advancing CKD stage. The following investigations are recommended:
Monitoring Frequency by CKD Stage
| CKD Stage | eGFR (mL/min/1.73 m²) | Frequency | Tests |
|---|---|---|---|
| Stage 2–3a | 45–89 | Every 6–12 months | Calcium, phosphate, PTH, 25(OH)D |
| Stage 3b | 30–44 | Every 3–6 months | Calcium, phosphate, PTH, 25(OH)D, ALP |
| Stage 4 | 15–29 | Every 1–3 months | Calcium, phosphate, PTH, 25(OH)D, ALP |
| Stage 5 / 5D | <15 / Dialysis | Monthly (or per dialysis unit protocol) | Calcium, phosphate, PTH, 25(OH)D, ALP |
Biochemical Targets Summary
| Parameter | CKD 3–4 Target | CKD 5D Target |
|---|---|---|
| Corrected Calcium | 2.10–2.55 mmol/L (normal range) | 2.10–2.55 mmol/L (normal range) |
| Phosphate | Within normal range (0.8–1.5 mmol/L) | 0.8–1.5 mmol/L |
| Intact PTH | Within normal range (1.6–7.2 pmol/L) | 2–9× ULN (~16–72 pmol/L)* |
| 25(OH) Vitamin D | ≥75 nmol/L | ≥75 nmol/L |
| Ca × P product | Minimise | <4.4 mmol²/L² |
*Assay-specific; consult local laboratory reference ranges. Avoid over-suppression of PTH below 2× ULN in CKD 5D due to adynamic bone disease risk.
Management — Phosphate Binders, Vitamin D, Cinacalcet
Management of CKD-MBD is guided by biochemical targets and involves a stepped approach: dietary phosphate restriction, phosphate binders, vitamin D supplementation, active vitamin D analogues, calcimimetics, and in refractory cases, parathyroidectomy.
Dietary Phosphate Restriction
Dietary phosphate intake should be limited to 800–1000 mg/day (25–32 mmol/day). Patients should be counselled to avoid phosphate-containing food additives (processed meats, soft drinks, preservatives) as inorganic phosphate additives are nearly 100% absorbed compared with 40–60% absorption from organic (food-bound) phosphate. A renal dietitian referral is recommended for all patients with CKD 4–5.
Phosphate Binders
Phosphate binders are the mainstay of hyperphosphataemia treatment. They must be taken with meals to bind dietary phosphate in the gut. Choice depends on calcium status, cost, tolerability, and vascular calcification risk.
Vitamin D Therapy
Vitamin D therapy in CKD-MBD addresses two separate deficits:
Native Vitamin D Replacement
Cholecalciferol (vitamin D₃) or ergocalciferol (vitamin D₂) should be given to all CKD patients with 25(OH)D <75 nmol/L.
Active Vitamin D Analogues
Active vitamin D analogues directly suppress PTH synthesis and are indicated when PTH is above target despite normalisation of phosphate and 25(OH)D.
Calcimimetics — Cinacalcet
Cinacalcet is a calcimimetic agent that allosterically activates the calcium-sensing receptor (CaSR) on parathyroid chief cells, increasing sensitivity to extracellular calcium and suppressing PTH secretion. It is indicated for secondary hyperparathyroidism in CKD 5D when PTH remains above target despite adequate phosphate binders and active vitamin D therapy.
Stepwise Management Algorithm
Calciphylaxis (Calcific Uremic Arteriolopathy)
Clinical Presentation & Diagnostic Criteria
CKD-MBD is typically identified through biochemical screening in patients with known CKD. Many patients are asymptomatic until advanced disease manifests with skeletal or cardiovascular complications.
Symptoms and Signs
- Bone pain (especially spine, hips, ribs)
- Proximal myopathy
- Pathological fractures
- Joint swelling (gouty-like in brown tumours)
- Brown tumours (cystic bone lesions in osteitis fibrosa)
- Subperiosteal erosions (radial side of middle phalanges)
- Vascular calcification (coronary, peripheral)
- Calciphylaxis (skin necrosis)
- Soft-tissue and periarticular calcification
- Corneal calcification
- Cardiovascular events (MI, stroke, heart failure)
- Metastatic calcification in viscera
Diagnostic Criteria (KDIGO 2017)
CKD-MBD is diagnosed when one or more of the following are present in a patient with CKD:
- Abnormalities of calcium, phosphate, PTH, or vitamin D metabolism
- Abnormalities in bone turnover, mineralisation, volume, linear growth, or strength (renal osteodystrophy)
- Vascular or other soft-tissue calcification
No single biochemical value establishes the diagnosis — a combination of serial measurements and trend analysis is required. Bone biopsy is the definitive test for renal osteodystrophy but is not required in routine clinical practice.
Risk Stratification & Severity Scoring
Risk in CKD-MBD is determined by the degree of biochemical derangement, presence of vascular calcification, bone disease type, and comorbid burden.
Monitoring
Ongoing monitoring is essential to guide therapy titration and detect complications. Key principles:
- Trend analysis over single values: PTH varies significantly between measurements; 3 consecutive values trending in the same direction are more informative than a single result.
- Adjust therapy based on trends, not isolated results.
- Monitor calcium and phosphate before and after every active vitamin D or cinacalcet dose change.
- 25(OH)D: Check at 3 months after initiating cholecalciferol, then every 6–12 months.
- Alkaline phosphatase: Track every 3–6 months; rising ALP suggests increasing bone turnover.
- Vascular calcification: Consider lateral abdominal X-ray at baseline in CKD 5/5D and repeat every 2–3 years or if clinical change.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2017;7(1):1–59.
- 2. Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease–mineral and bone disorder (CKD-MBD). Kidney Int Suppl. 2009;(113):S1–130.
- 3. Australia and New Zealand Dialysis and Transplant Registry. ANZDATA 46th Annual Report 2023 (Data to 2022). Adelaide: ANZDATA; 2023. Available from: https://www.anzdata.org.au
- 4. Elder GJ, Sherrard DJ. Calcium, phosphate, and vitamin D in chronic kidney disease. In: Turner N, editor. Textbook of Renal Disease. 2nd ed. Melbourne: Elsevier; 2020. p. 312–335.
- 5. Isakova T, Nickolas TL, Denburg M, et al. KDOQI US Commentary on the 2017 KDIGO Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease–Mineral and Bone Disorder (CKD-MBD). Am J Kidney Dis. 2017;70(6):737–751.
- 6. RACGP. Guidelines for Preventive Activities in General Practice. 9th ed. East