📋 Key Information Summary
- Nephrolithiasis affects ~10% of Australians, with recurrence rates up to 50% within 10 years without preventive strategies.
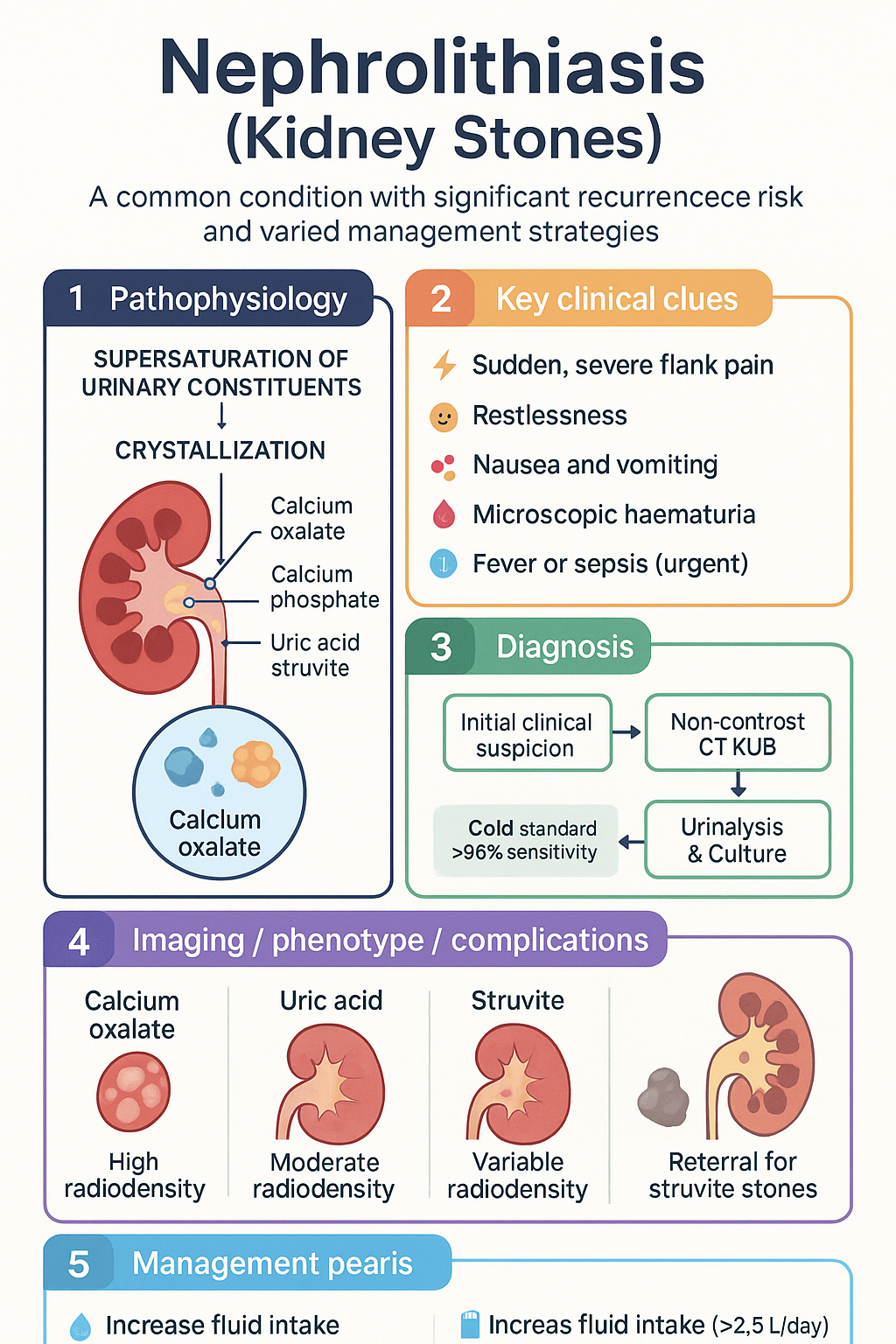
- Calcium oxalate/phosphate stones account for 70–80% of cases; uric acid, struvite, and cystine stones are less common.
- Non-contrast CT KUB is the gold-standard investigation for acute flank pain, with >95% sensitivity for stones >2 mm.
- First presentation or high-risk stones warrant a 24-hour urine metabolic work-up to guide specific prevention.
- Management is guided by stone size, location, composition, and degree of obstruction.
- Medical expulsive therapy with tamsulosin 400 mcg daily for up to 4 weeks is first-line for distal ureteric stones ≤10 mm.
- Shockwave lithotripsy (SWL) is first-line for renal stones <20 mm and proximal ureteric stones <10 mm.
- Ureteroscopy with laser lithotripsy has higher stone-free rates than SWL for most ureteric stones and renal stones <20 mm.
- Struvite (infection) stones require complete surgical removal and targeted antibiotic therapy to prevent recurrence.
- All patients should receive fluid intake advice (>2.5 L/day) and dietary modification based on stone composition.
- Aboriginal and Torres Strait Islander peoples have higher rates of renal disease and may face barriers to timely specialist care.
Introduction & Australian Epidemiology
Nephrolithiasis (kidney stone disease) is a common and painful condition characterised by the formation of hard mineral and salt deposits within the urinary tract. In Australia, the lifetime prevalence is approximately 10–15%, with a male-to-female ratio of 3:1. The peak incidence is between ages 30–60 years.
Recurrence is a major concern, with ~50% of patients experiencing a recurrence within 10 years without preventive intervention. The economic burden is significant, encompassing emergency presentations, surgical procedures, and lost productivity.
Stone composition varies, with calcium-based stones (oxalate and phosphate) predominating. Accurate diagnosis, identification of modifiable risk factors, and appropriate acute management are essential to reduce morbidity and prevent long-term recurrence.
Stone Types & Pathophysiology
Stone formation (lithogenesis) occurs when urinary constituents supersaturate and crystallise. Key factors include urine volume, pH, and the concentration of stone-forming salts and inhibitors.
Major Stone Types
| Stone Type | Frequency | Key Associations | Radiodensity (CT) |
|---|---|---|---|
| Calcium Oxalate | ~70% | Hypercalciuria, hyperoxaluria, low urine volume, hypocitraturia | High (bright white) |
| Calcium Phosphate | ~10–15% | Renal tubular acidosis, hyperparathyroidism | High |
| Uric Acid | ~10% | Acidic urine (pH <5.5), gout, metabolic syndrome | Moderate (less dense) |
| Struvite (Infection) | ~5–10% | Urease-producing bacteria (e.g., Proteus, Klebsiella) | Variable |
| Cystine | ~1% | Autosomal recessive defect in dibasic amino acid transport | Moderate |
Clinical Features & Diagnosis
Clinical Presentation
- Classic renal colic: Sudden, severe, colicky flank pain radiating to the groin or labia/testis. Patient is typically restless and unable to find a comfortable position.
- Associated nausea, vomiting, and haematuria (microscopic in ~80%).
- Signs of obstruction or infection: fever, rigors, sepsis, or anuria (bilateral obstruction) require urgent intervention.
Diagnostic Investigations
Metabolic Work-up & Risk Factors
Indications for Metabolic Evaluation
- First-time stone formers with high-risk features (family history, solitary kidney, chronic diarrhoea, obesity, diabetes).
- All recurrent stone formers.
- Patients with struvite or cystine stones.
24-Hour Urine Collection
The cornerstone of metabolic work-up. Two collections are recommended on unrestricted diet.
| Parameter | Normal Range | Clinical Significance |
|---|---|---|
| Volume | >2.5 L/day | Low volume increases supersaturation risk |
| Calcium | <6.2 mmol/day (women) <7.5 mmol/day (men) |
Hypercalciuria is the most common abnormality |
| Oxalate | <0.46 mmol/day | Elevated in primary hyperoxaluria or high-oxalate diet |
| Citrate | >1.9 mmol/day (women) >2.5 mmol/day (men) |
Hypocitraturia promotes calcium stone formation |
| Urate | <4.5 mmol/day | Can promote calcium or uric acid stones |
| pH | 5.8–6.2 | Persistently low (<5.5) favours uric acid; high (>6.2) favours phosphate |
Common Modifiable Risk Factors
Management
Acute Renal Colic Management
Definitive Management by Stone Size & Location
Medical Prevention by Stone Type
Special Populations
📚 References
- 1. Australian Institute of Health and Welfare (AIHW). Kidney stones in Australia. Canberra: AIHW; 2023.
- 2. The Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice (Red Book). 10th ed. East Melbourne: RACGP; 2023.
- 3. Urological Society of Australia and New Zealand (USANZ). Position statement on the management of ureteric calculi. BJU Int. 2022;129(5):611-620.
- 4. Kidney Health Australia. Chronic kidney disease (CKD) management in primary care. 4th ed. Melbourne: Kidney Health Australia; 2020.
- 5. National Health and Medical Research Council (NHMRC). Australian guidelines to reduce health risks from drinking alcohol. Canberra: NHMRC; 2020.
- 6. Turnbull D, et al. Medical expulsive therapy for ureteric stones: a systematic review and meta-analysis. Med J Aust. 2021;214(8):375-381.
- 7. Turk C, et al. EAU Guidelines on Diagnosis and Conservative Management of Urolithiasis. Eur Urol. 2022;82(3):284-299.
- 8. Pearle MS, et al. AUA/CUA/SUFU Guideline: Surgical Management of Stones. J Urol. 2016;196(4):1153-1160.
- 9. Aboriginal and Torres Strait Islander Health Performance Framework. Kidney health. Australian Institute of Health and Welfare; 2023.
- 10. Moe OW. Kidney stones: pathophysiology and medical management. Lancet. 2006;367(9507):333-344.
- 11. Services Australia. Medicare Benefits Schedule (MBS) Item 56001, 58505. Canberra: Australian Government; 2024.
- 12. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.