📋 Key Information Summary
- Diabetic nephropathy (DN) is the leading cause of end-stage renal failure (ESRF) in Australia, accounting for approximately 30–40% of incident dialysis patients.
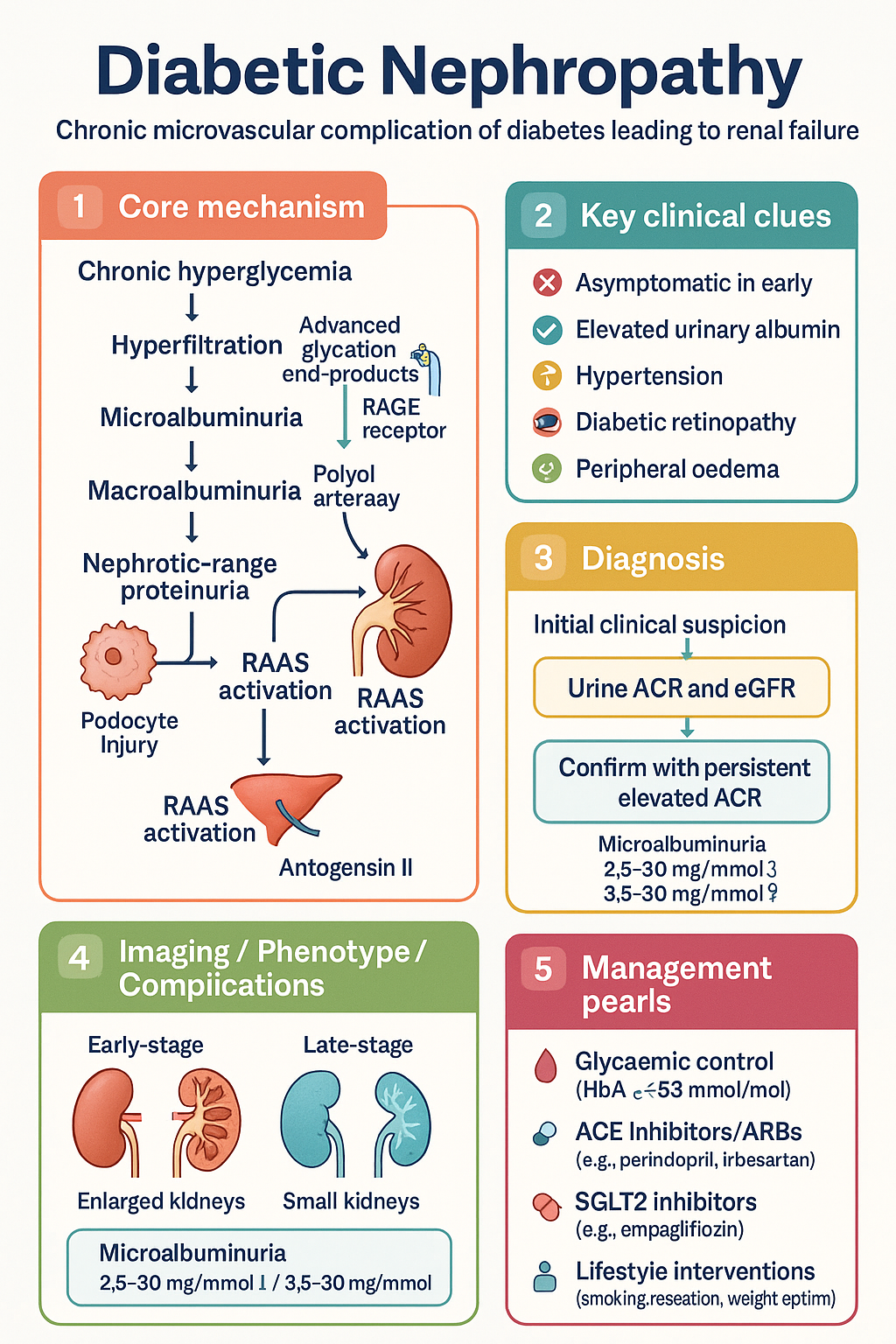
- DN progresses through five stages: hyperfiltration → silent/microalbuminuria → macroalbuminuria → nephrotic-range proteinuria → ESRF.
- Annual screening with urine albumin-to-creatinine ratio (ACR) and estimated glomerular filtration rate (eGFR) is mandatory from diagnosis in type 2 diabetes and from 5 years post-diagnosis in type 1 diabetes.
- Glycaemic target HbA1c ≤53 mmol/mol (7.0%) reduces microvascular complications; individualise targets in advanced CKD to avoid hypoglycaemia.
- ACE inhibitors (e.g. perindopril, ramipril) or ARBs (e.g. irbesartan, telmisartan) are first-line renoprotective agents — titrate to maximum tolerated dose.
- SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin) provide independent renoprotection and reduce CKD progression by 30–40%; initiate if eGFR ≥20 mL/min/1.73 m².
- Finerenone (Kerendia®), a non-steroidal mineralocorticoid receptor antagonist, further reduces kidney and cardiovascular events in DN with persistent albuminuria — requires close potassium monitoring.
- Blood pressure target ≤130/80 mmHg (≤125/75 if ACR >30 mg/mmol) — use combination therapy as needed.
- Lipid management with high-intensity statin (e.g. atorvastatin 40–80 mg) is recommended for all patients with DN and CKD stages 3–5.
- Refer to nephrology if eGFR <30 mL/min/1.73 m², rapid eGFR decline (>5 mL/min/year), refractory hyperkalaemia, or diagnostic uncertainty.
- Aboriginal and Torres Strait Islander peoples experience DN at 3–4× the rate of non-Indigenous Australians with earlier onset and faster progression.
- Smoking cessation, weight optimisation (BMI <30), dietary sodium restriction (<6 g NaCl/day), and regular exercise are essential lifestyle interventions.
- Avoid nephrotoxins — minimise NSAID use, adjust metformin dose when eGFR <45, discontinue metformin if eGFR <15.
Introduction & Australian Epidemiology
Diabetic nephropathy (DN) is a chronic microvascular complication of diabetes mellitus characterised by progressive albuminuria, systemic hypertension, and a relentless decline in glomerular filtration rate (GFR). It is the single leading cause of end-stage renal failure (ESRF) requiring renal replacement therapy (RRT) in Australia and other developed nations.
In Australia, approximately 1.3 million people live with diabetes (primarily type 2), and DN accounts for roughly 30–40% of all incident patients commencing dialysis or kidney transplantation each year. The Australian Institute of Health and Welfare (AIHW) reports that CKD attributable to diabetes has increased steadily over the past two decades, reflecting rising type 2 diabetes prevalence, improved survival in other CKD aetiologies, and increasing recognition of early-stage disease.
DN carries significant cardiovascular morbidity — patients with albuminuria have a 2- to 4-fold increased risk of myocardial infarction, stroke, and cardiovascular death compared with diabetic patients without nephropathy. The economic burden is substantial, with dialysis alone costing approximately ,000–0,000 AUD per patient per year.
Landmark trials — RENAAL, IDNT, ADVANCE, EMPA-KIDNEY, DAPA-CKD, and FIDELIO/FIGARO — have established a multi-targeted approach to DN management, combining glycaemic optimisation, RAAS blockade, SGLT2 inhibition, non-steroidal MRA therapy, and aggressive cardiovascular risk modification. This guideline synthesises current evidence for Australian primary care and specialist practice.
Pathophysiology & Stages (Microalbuminuria to ESRF)
DN arises from the cumulative effects of chronic hyperglycaemia on the glomerular microvasculature, tubulointerstitium, and systemic vasculature. The pathogenesis is multifactorial and involves haemodynamic, metabolic, inflammatory, and fibrotic pathways.
Key Pathogenic Mechanisms
- Glomerular hyperfiltration: Hyperglycaemia induces afferent arteriolar vasodilation and efferent arteriolar constriction (mediated by angiotensin II), raising intraglomerular pressure and GFR. This causes mechanical stress on podocytes and the glomerular basement membrane (GBM).
- Advanced glycation end-products (AGEs): Non-enzymatic glycation of proteins activates the RAGE receptor, promoting inflammation, oxidative stress, and mesangial matrix expansion.
- Polyol and hexosamine pathways: Excess glucose flux generates sorbitol (via aldose reductase) and glucosamine metabolites, contributing to osmotic stress and altered gene expression.
- Podocyte injury: Loss of nephrin and podocin expression leads to foot process effacement and protein leak across the slit diaphragm.
- Tubulointerstitial fibrosis: Progressive tubular atrophy, interstitial inflammation, and fibrosis correlate more closely with declining GFR than glomerular changes alone.
- RAAS activation: Local and systemic RAAS over-activation perpetuates glomerular hypertension, fibrosis, and sodium retention.
Stages of Diabetic Nephropathy
| Stage | Description | ACR (mg/mmol) | eGFR (mL/min/1.73 m²) | Duration to Progression |
|---|---|---|---|---|
| 1 — Hyperfiltration | Enlarged kidneys, elevated GFR, normal albumin excretion | <2.5 (♂) / <3.5 (♀) | >120 (often) | Years |
| 2 — Silent stage | GBM thickening, mesangial expansion; normal ACR and GFR | Normal | Normal | Variable |
| 3 — Microalbuminuria | Incipient nephropathy; earliest clinical detection possible | 2.5–30 (♂) / 3.5–30 (♀) | Normal–mildly reduced | 5–15 years to macro |
| 4 — Macroalbuminuria | Overt nephropathy; progressive GFR decline | >30 | Declining (often 30–60) | 5–10 years to ESRF |
| 5 — ESRF | End-stage renal failure; dialysis or transplant required | Variable (may fall as GFR drops) | <15 | — |
Clinical Features & Screening
Clinical Features by Stage
Early DN is clinically silent — the only detectable abnormality is elevated urinary albumin. Symptoms develop insidiously as nephropathy progresses.
Screening Recommendations (Australian Guidelines)
- Type 2 diabetes: Screen at diagnosis and at least annually thereafter (RACGP / Diabetes Australia).
- Type 1 diabetes: Screen from 5 years after diagnosis and at least annually.
- Screening test: Spot urine albumin-to-creatinine ratio (ACR) — preferred over 24-hour urine collection.
- Confirmatory testing: Persistently elevated ACR on 2 of 3 samples over ≥3 months (exclude transient causes: UTI, acute illness, exercise, menstruation, haematuria).
- eGFR: Calculate using CKD-EPI 2021 equation (creatinine-based, without race coefficient) at each screening visit.
Investigations (eGFR, ACR, Biopsy Rarely)
Investigations in DN serve to detect early disease, stage CKD, exclude alternative diagnoses, and monitor progression.
Core Investigations
CKD Staging (KDIGO Heat Map)
| eGFR Stage | A1 (Normal–mild ↑) | A2 (Moderately ↑) | A3 (Severely ↑) |
|---|---|---|---|
| G1 ≥90 | Green | Yellow | Orange |
| G2 60–89 | Green | Yellow | Orange |
| G3a 45–59 | Yellow | Orange | Red |
| G3b 30–44 | Orange | Red | Red |
| G4 15–29 | Red | Red | Red |
| G5 <15 | Red | Red | Red |
Management (Glycaemic Control, ACEi/ARB, SGLT2i, Finerenone)
Management of DN requires a multi-pronged approach addressing glycaemia, blood pressure, albuminuria, cardiovascular risk, and lifestyle factors simultaneously. Each intervention has additive benefit.
1. Glycaemic Control
Intensive glycaemic control slows the onset and progression of microalbuminuria and retinopathy (UKPDS, DCCT/EDIC, ADVANCE). The benefits on established macroalbuminuria are more modest.
2. RAAS Blockade — ACE Inhibitors & ARBs
ACEi and ARBs reduce intraglomerular pressure, lower proteinuria, slow GFR decline, and reduce cardiovascular events. They are the cornerstone of renoprotective therapy in DN.
3. SGLT2 Inhibitors
SGLT2 inhibitors have emerged as a transformative therapy for DN, providing renoprotection independent of and additive to glycaemic control. The EMPA-KIDNEY, DAPA-CKD, and CREDENCE trials demonstrated 30–40% reductions in composite kidney endpoints.
4. Finerenone — Non-Steroidal MRA
Finerenone is a selective non-steroidal mineralocorticoid receptor antagonist that reduces inflammation and fibrosis in the kidney and heart with a lower risk of gynaecomastia and hyperkalaemia compared with spironolactone.
5. Blood Pressure Management
Hypertension accelerates DN progression. Tight blood pressure control reduces albuminuria and slows GFR decline.
- Target: ≤130/80 mmHg (general DN); ≤125/75 mmHg if ACR >30 mg/mmol (per KDIGO and Australian guidelines).
- First-line: ACEi or ARB (renoprotective beyond BP lowering).
- Second-line add-on: Amlodipine (calcium channel blocker) or indapamide (thiazide-like diuretic).
- Loop diuretic: Furosemide preferred over thiazides if eGFR <30 mL/min.
- Sodium restriction: <6 g NaCl/day (≈2.3 g sodium) — reduces proteinuria and enhances ACEi efficacy.
6. Lipid Management
Cardiovascular disease is the leading cause of death in DN. All patients with DN and CKD stages 3–5 should receive lipid-lowering therapy.
7. Antiplatelet Therapy
Low-dose aspirin (75–100 mg daily) is recommended for secondary prevention in patients with established CVD. Primary prevention should be individualised (bleeding vs. cardiovascular risk).
8. Smoking Cessation
Smoking doubles the risk of DN progression and ESRF. All patients should be offered pharmacotherapy (varenicline, NRT) and behavioural support. Quitline: 13 78 48.
Monitoring
Regular monitoring is essential to detect progression, titrate medications, and manage complications.
| Parameter | Frequency | Notes |
|---|---|---|
| ACR + eGFR | Every 6–12 months (stable); every 3 months if declining | Confirm persistent albuminuria with repeat testing |
| Serum potassium | 1–2 weeks after ACEi/ARB initiation or dose change; every 3–6 months thereafter | More frequently if on finerenone (1 wk, 4 wk, then monthly) |
| Serum creatinine | With each eGFR check | Expect 10–20% rise after ACEi/ARB start — acceptable if <30% and stabilises |
| HbA1c | Every 3–6 months | May be unreliable in ESRF; use fructosamine or CGM data if available |
| Blood pressure | Each visit; consider ABPM if white-coat suspected | Home BP monitoring encouraged |
| Lipids | Annually (or 6–8 weeks after statin initiation) | Non-fasting acceptable |
| FBE, iron studies | Every 6 months if CKD stage 3b+ | Anaemia of CKD — consider EPO if Hb <100 g/L |
| Calcium, phosphate, PTH | Annually from CKD 3b; more often CKD 4–5 | CKD-mineral bone disorder management |
| Retinal screening | Every 1–2 years | Supports DN diagnosis; concurrent retinopathy common |
| Foot examination | Annually (more if risk factors) | Peripheral neuropathy + PAD screening |
When to Refer to Nephrology
- eGFR <30 mL/min/1.73 m² (CKD stage 4)
- Rapid eGFR decline: >5 mL/min/year sustained
- Refractory hyperkalaemia (K⁺ >5.5 despite intervention)
- Resistant hypertension (≥4 agents at maximally tolerated doses)
- Nephrotic syndrome without typical diabetic pattern
- Suspected non-diabetic kidney disease
- RRT planning — AV fistula creation should occur 6–12 months before anticipated dialysis
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. KDIGO 2024 Clinical Practice Guideline for Evaluation and Management of Chronic Kidney Disease. Kidney International. 2024;105(4S):S117–S314.
- 2. Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy (CREDENCE). N Engl J Med. 2019;380(24):2295–2306.
- 3. Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in Patients with Chronic Kidney Disease (DAPA-CKD). N Engl J Med. 2020;383(15):1436–1446.
- 4. The EMPA-KIDNEY Collaborative Group. Empagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2023;388(2):117–127.
- 5. Bakris GL, Agarwal R, Anker SD, et al. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes (FIDELIO-DKD). N Engl J Med. 2020;383(23):2219–2229.
- 6. Filippatos G, Anker SD, Agarwal R, et al. Finerenone and Cardiovascular Outcomes in Patients with Chronic Kidney Disease and Type 2 Diabetes (FIGARO-DKD). Circulation. 2021;143(6):540–552.
- 7. Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of Losartan on Renal and Cardiovascular Outcomes in Patients with Type 2 Diabetes and Nephropathy (RENAAL). N Engl J Med. 2001;345(12):861–869.
- 8. Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective Effect of the Angiotensin-Receptor Antagonist Irbesartan in Patients with Nephropathy Due to Type 2 Diabetes (IDNT). N Engl J Med. 2001;345(12):851–860.
- 9. Australian Institute of Health and Welfare. Chronic kidney disease: Australian facts. AIHW, Canberra. 2023.
- 10. RACGP / Diabetes Australia. General practice management of type 2 diabetes 2016–2018 (updated 2020). The Royal Australian College of General Practitioners, Melbourne.
- 11. Kidney Health Australia. Chronic Kidney Disease (CKD) Management in Primary Care. 4th edition. Melbourne: Kidney Health Australia; 2020.
- 12. Heart Foundation of Australia. Position statement: Management of hypertension in adults with type 2 diabetes. 2023.
- 13. RHDAustralia (ARF/RHD writing group). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd edition. Menzies School of Health Research, Darwin.
- 14. National Aboriginal Community Controlled Health Organisation (NACCHO). Aboriginal and Torres Strait Islander chronic disease resources. NACCHO, Canberra.