📋 Key Information Summary
- Normal serum potassium (K⁺) is 3.5–5.0 mmol/L; values outside this range require urgent clinical assessment and serial ECG monitoring.
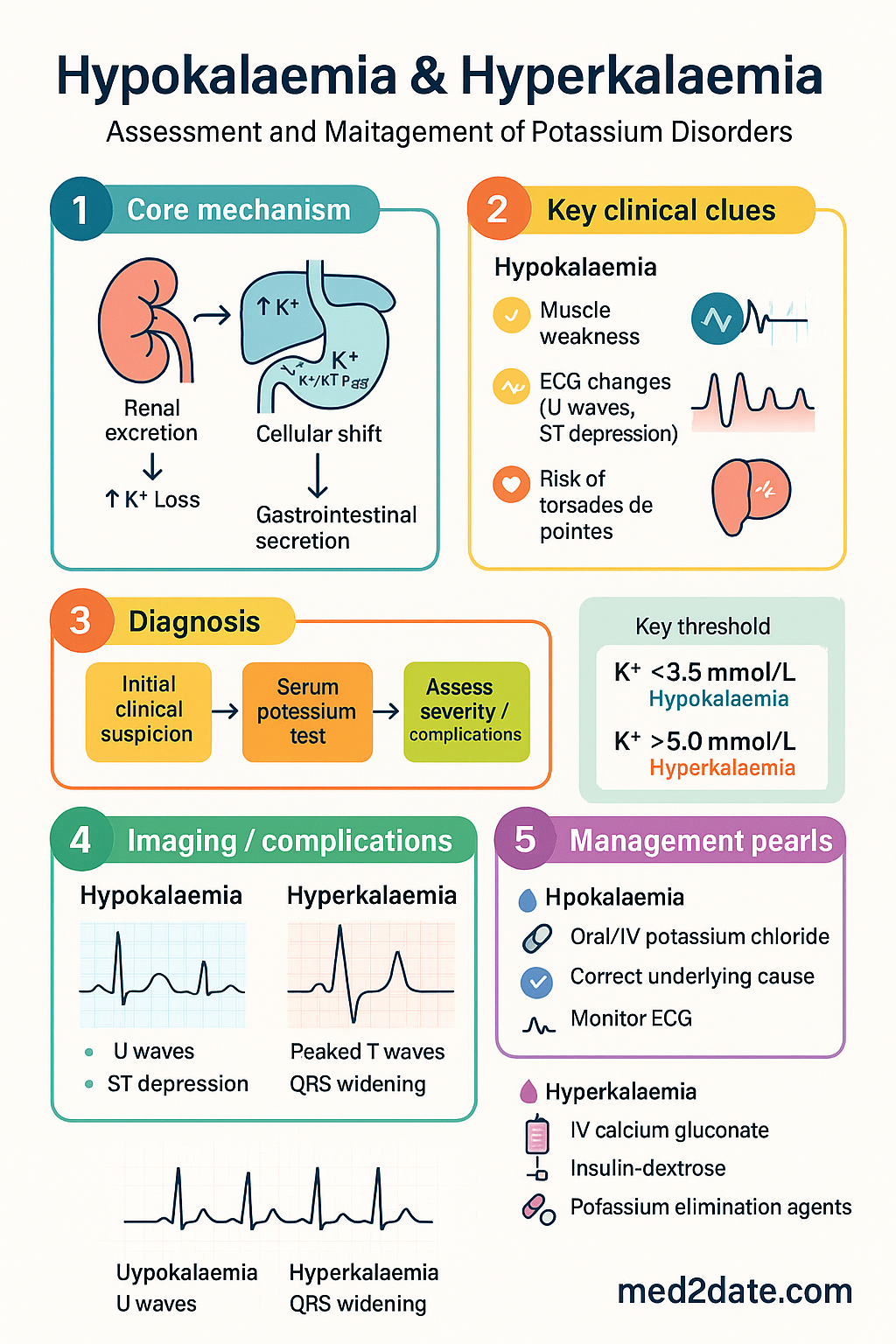
- Hypokalaemia (K⁺ <3.5 mmol/L) causes characteristic ECG changes including U waves, ST depression, T-wave flattening, and increased risk of torsades de pointes.
- The most common causes of hypokalaemia are diuretic therapy (frusemide, thiazides), gastrointestinal losses (vomiting, diarrhoea), and renal tubular disorders.
- Oral potassium chloride (KCl) is first-line for mild–moderate hypokalaemia; IV KCl is reserved for severe hypokalaemia (K⁺ <2.5 mmol/L), symptomatic patients, or those unable to tolerate oral replacement.
- IV KCl must be administered at ≤20 mmol/hour via infusion pump in normal saline or glucose-free solution; concentrations >40 mmol/L require a central line and cardiac monitoring.
- Hyperkalaemia (K⁺ >5.0 mmol/L) is a medical emergency when K⁺ >6.5 mmol/L or ECG changes are present; it may cause fatal ventricular fibrillation without warning.
- ECG signs of hyperkalaemia progress from peaked T waves → PR prolongation → QRS widening → loss of P waves → sine-wave pattern → asystole/VF.
- The hyperkalaemia emergency protocol prioritises myocardial membrane stabilisation (IV calcium gluconate 10%, 10 mL over 10 min) before potassium-lowering measures.
- Insulin-dextrose (Actrapid 10 units + 50 mL 50% glucose IV over 15–30 min) shifts potassium intracellularly and lowers serum K⁺ by 0.5–1.2 mmol/L within 30–60 minutes.
- Sodium polystyrene sulfonate (Resonium A®) or calcium resonium provides enteral potassium elimination over 1–6 hours; patiromer and sodium zirconium cyclosilicate are newer agents.
- All patients with severe hypokalaemia or hyperkalaemia require continuous cardiac telemetry and serial potassium monitoring every 1–2 hours until stable.
- Aboriginal and Torres Strait Islander peoples experience a higher burden of chronic kidney disease and thus potassium disorders; culturally safe management and remote-area protocols are essential.
Introduction & Australian Epidemiology
Potassium is the principal intracellular cation, with approximately 98% of total body potassium located within cells and only 2% in the extracellular fluid. The narrow normal serum potassium range of 3.5–5.0 mmol/L is tightly regulated by renal excretion, cellular shift mechanisms (primarily insulin- and catecholamine-mediated), and gastrointestinal secretion. Disruptions in potassium homeostasis are common in clinical practice and may be rapidly life-threatening — particularly hyperkalaemia, which can precipitate fatal ventricular fibrillation without preceding warning symptoms.
In Australia, electrolyte disturbances are among the most frequently encountered laboratory abnormalities. Hypokalaemia is identified in approximately 20% of hospitalised patients, while hyperkalaemia affects up to 10% of admissions, with markedly higher prevalence among patients with chronic kidney disease (CKD), heart failure, and those taking renin–angiotensin–aldosterone system (RAAS) inhibitors or potassium-sparing diuretics.
The Australian Institute of Health and Welfare (AIHW) reports that CKD — a leading driver of hyperkalaemia — affects approximately 1 in 10 Australians, with disproportionate burden in Aboriginal and Torres Strait Islander communities. With an ageing population, rising prevalence of diabetes mellitus, and widespread use of RAAS blockade for cardiorenal protection, the clinical significance of potassium disorders in Australian practice continues to grow.
This guideline provides a comprehensive, evidence-based approach to the assessment and management of both hypokalaemia and hyperkalaemia in Australian clinical settings, incorporating PBS-listed therapies, standard emergency protocols, and considerations for special populations.
Hypokalaemia: Causes & ECG Changes
Definition & Severity Classification
Causes of Hypokalaemia
The differential diagnosis is approached by mechanism: reduced intake, intracellular shift, or increased losses (renal or gastrointestinal).
| Mechanism | Examples | Clinical Clues |
|---|---|---|
| Inadequate intake | Starvation, anorexia nervosa, alcoholism, clay ingestion | Low dietary potassium; often chronic and mild |
| Intracellular shift | Insulin therapy, β₂-agonists (salbutamol), alkalosis, hypothermia, thyrotoxic periodic paralysis | Acute onset; total body K⁺ may be normal |
| Renal losses | Loop diuretics (frusemide), thiazide diuretics, amphotericin B, renal tubular acidosis (Type 1 & 2), hypomagnesaemia, primary hyperaldosteronism, Gitelman syndrome, Bartter syndrome | Spot urine K⁺ >20 mmol/L; metabolic alkalosis often present |
| GI losses | Vomiting, nasogastric drainage, diarrhoea, laxative abuse, villous adenoma | Spot urine K⁺ <20 mmol/L; diarrhoea causes hyperchloraemic metabolic acidosis; vomiting causes metabolic alkalosis |
| Skin losses | Excessive sweating, burns, cystic fibrosis | Usually mild unless extreme |
ECG Changes in Hypokalaemia
ECG changes correlate imperfectly with serum potassium levels but are critical for risk assessment:
- Early: T-wave flattening and U-wave prominence (U wave >T wave in same lead)
- Moderate: ST-segment depression, prolonged QT interval (actually QU interval), T–U fusion
- Severe: Prominent U waves, ventricular ectopy, torsades de pointes (polymorphic VT), ventricular fibrillation
The U wave is the hallmark ECG finding in hypokalaemia — best seen in leads V₂–V₄. Concurrent hypomagnesaemia increases arrhythmia risk independently and must always be checked and corrected.
Hypokalaemia Management (IV/Oral KCl, Treat Cause)
General Principles
- Always identify and treat the underlying cause (e.g., cease offending diuretic, treat diarrhoea, correct hypomagnesaemia).
- Concurrent hypomagnesaemia must be corrected — refractory hypokalaemia will not resolve until magnesium is replete.
- Oral replacement is preferred whenever feasible due to safety and efficacy.
- A 20 mmol oral KCl dose raises serum K⁺ by approximately 0.1–0.2 mmol/L in patients with normal renal function.
- Maximum recommended IV KCl infusion rate: 20 mmol/hour via peripheral line; 40 mmol/hour via central line with continuous telemetry in ICU.
Pharmacotherapy
Additional Agents for Refractory Hypokalaemia
- Magnesium replacement: Magnesium sulfate 1–2 g IV over 1–2 hours (or 600 mg PO TDS as MgO). Check serum Mg²⁺ — target ≥0.7 mmol/L. Without magnesium repletion, potassium correction will be refractory.
- Spironolactone / Eplerenone: In hyperaldosteronism-mediated hypokalaemia, potassium-sparing diuretics can help maintain K⁺ within normal range.
- Amiloride: 5–10 mg PO daily; useful in Gitelman syndrome and lithium-induced nephrogenic diabetes insipidus with potassium wasting.
Treatment Algorithm
Hyperkalaemia: Causes & ECG Changes
Definition & Severity Classification
Causes of Hyperkalaemia
| Mechanism | Examples | Clinical Clues |
|---|---|---|
| Reduced renal excretion | CKD (GFR <30), acute kidney injury, Type 4 RTA, potassium-sparing diuretics (spironolactone, amiloride, eplerenone), RAAS inhibitors (ACEi, ARB, direct renin inhibitors), NSAIDs, trimethoprim | Most common cause; check eGFR and medication reconciliation |
| Transcellular shift (out of cells) | Metabolic acidosis, insulin deficiency (DKA), β-blockers (non-selective), digitalis toxicity, succinylcholine, hyperosmolality, tissue necrosis (rhabdomyolysis, burns, tumour lysis syndrome, severe trauma) | Acute rise; total body K⁺ may be normal or low |
| Excessive intake | IV KCl excess, salt substitutes (KCl-based), massive blood transfusion, potassium-rich diet in setting of impaired renal function | Rarely causes hyperkalaemia alone without impaired excretion |
| Pseudohyperkalaemia | Haemolysed sample, prolonged tourniquet/clenching, severe thrombocytosis (>500 × 10⁹/L), severe leucocytosis (>100 × 10⁹/L) | Repeat sample with minimal tourniquet time; plasma K⁺ vs serum K⁺ may help differentiate |
| Adrenal insufficiency | Primary adrenal failure (Addison disease), congenital adrenal hyperplasia, heparin therapy | Hyperkalaemia + hyponatraemia + hypotension is the classic triad |
ECG Changes in Hyperkalaemia
ECG changes are the most important bedside indicator of hyperkalaemia severity and the need for emergent treatment. Changes progress in a predictable sequence:
Hyperkalaemia Emergency Management
The emergency management of hyperkalaemia follows a structured protocol targeting three goals: (1) myocardial membrane stabilisation, (2) intracellular potassium shift, and (3) total body potassium elimination. All three measures should be initiated simultaneously in severe hyperkalaemia.
Immediate Emergency Protocol
Pharmacotherapy — Emergency Agents
Newer Potassium-Binding Agents
| Agent | Dose | Onset | PBS Status | Notes |
|---|---|---|---|---|
| Patiromer (Veltassa®) | 8.4 g PO daily | 7 hours | ✘ Not PBS listed | For chronic hyperkalaemia in CKD on RAAS blockade; TGA-approved; separate from other oral medications by 3 hours |
| Sodium Zirconium Cyclosilicate (Lokelma®) | 10 g PO TDS (acute); 5–10 g daily (maintenance) | 1–6 hours | ✘ Not PBS listed | Faster onset than patiromer; TGA-approved; sodium load — use with caution in heart failure |
Definitive Therapy — Haemodialysis
Ongoing Monitoring & Disposition
- Repeat serum K⁺ at 1 hour, 2 hours, and 4 hours post-treatment, then 6–hourly until stable.
- Continuous cardiac telemetry for minimum 6 hours after K⁺ normalisation (rebound hyperkalaemia common).
- Monitor blood glucose every 30 min for 2 hours post insulin-dextrose; maintain glucose >4.0 mmol/L.
- Identify and cease offending medications (ACEi/ARB, spironolactone, NSAIDs, trimethoprim, potassium supplements).
- Treat underlying cause (rhabdomyolysis, DKA, AKI).
Investigations
Monitoring
| Scenario | K⁺ Monitoring Frequency | ECG Monitoring | Glucose Monitoring |
|---|---|---|---|
| Mild hypokalaemia (outpatient) | Repeat in 24–48 hours | 12-lead ECG at baseline | Not required |
| Moderate–severe hypokalaemia (IV KCl) | Every 2–4 hours during infusion | Continuous telemetry | Not required unless diabetic |
| Mild–moderate hyperkalaemia (no ECG changes) | Every 2–4 hours until <5.5 | Telemetry recommended | Not required unless insulin given |
| Severe hyperkalaemia (emergency treatment) | Every 1 hour for 4 hours, then every 2 hours | Continuous telemetry — minimum 6 hours post-normalisation | Every 30 min for 2 hours post insulin-dextrose; then hourly × 6 hours |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Mount DB. Disorders of potassium balance. In: Skorecki K, Chertow GM, Marsden PA, Yu ASL, Taal MW, eds. Brenner and Rector's The Kidney. 11th ed. Philadelphia: Elsevier; 2020:595–630.
- 2. Kardalas E, Paschou SA, Anagnostis P, Muscogiuri G, Siasos G, Katsiki N. Hypokalaemia: a clinical update. Endocr Connect. 2018;7(4):R135–R146. doi:10.1530/EC-18-0109
- 3. Elliott MJ, Ronksley PE, Clase CM, Ahmed SB, Hemmelgarn BR. Management of patients with acute hyperkalaemia. CMAJ. 2010;182(15):1631–1635. doi:10.1503/cmaj.100461
- 4. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. AIHW, Canberra; 2023. Cat. no. PHE 229.
- 5. Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024;105(4S):S117–S314.
- 6. RACGP. Management of type 2 diabetes: a handbook for general practice. Royal Australian College of General Practitioners, East Melbourne; 2020.
- 7. Palmer BF, Clegg DJ. Diagnosis and treatment of hyperkalaemia. Cleve Clin J Med. 2017;84(12):939–944. doi:10.3949/ccjm.84a.17016
- 8. National Blood Authority Australia. A patient blood management guideline for adults with critical bleeding. 2nd ed. Canberra: NBA; 2023.
- 9. RHDAustralia (RHD Australia, the Menzies School of Health Research, the National Heart Foundation of Australia). The 2020 Australian guideline for prevention, diagnosis and management of acute rheumatic fever and rheumatic heart disease. 3rd ed. Darwin: Menzies School of Health Research; 2020.
- 10. Rossignol P, Legrand M, Kosiborod M, et al. Emergency management of severe hyperkalaemia: guideline for best practice and opportunities for the future. Pharmacol Res. 2016;113(Pt A):585–591. doi:10.1016/j.phrs.2016.09.039
- 11. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd ed. Sydney: ACSQHC; 2021.
- 12. Pharmaceuticals Benefits Scheme (PBS). PBS Schedule — Australian Government Department of Health. Available at: https://www.pbs.gov.au. Accessed 2024.