📋 Key Information Summary
- Cryoglobulinaemia is defined by the presence of immunoglobulins that reversibly precipitate at temperatures below 37°C and redissolve on rewarming.
- Three types: Type I (monoclonal, associated with haematological malignancy), Type II (mixed, monoclonal + polyclonal, strongly HCV-associated), Type III (mixed, polyclonal, often HCV or autoimmune).
- Type II and III (mixed) cryoglobulins account for >80% of cases in Australia and cause immune complex-mediated membranoproliferative glomerulonephritis (MPGN).
- Hepatitis C virus (HCV) is the driving aetiology in 80–90% of mixed cryoglobulinaemia cases; HCV serology and RNA testing is mandatory in all patients.
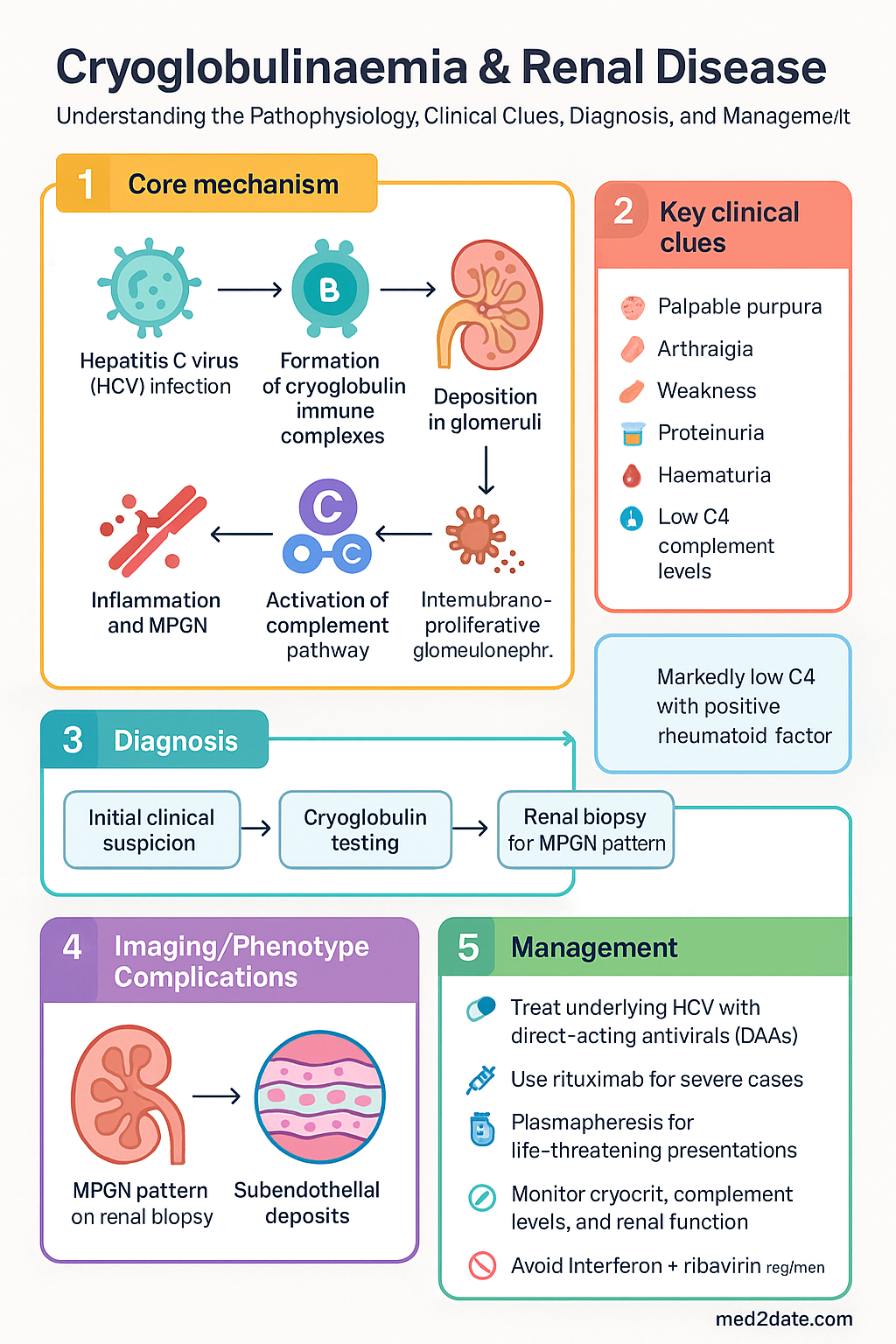
- Renal involvement presents as proteinuria, haematuria, and declining eGFR; renal biopsy shows MPGN pattern with subendothelial deposits and double contours on silver stain.
- Meltzer triad (palpable purpura, arthralgia, weakness) is the classic clinical presentation of mixed cryoglobulinaemic vasculitis.
- First-line renal disease management: treat underlying HCV with direct-acting antivirals (DAAs) — PBS-subsidised glecaprevir/pibrentasvir (Maviret®) or sofosbuvir/velpatasvir (Epclusa®).
- Rituximab (Mabthera®) is second-line immunosuppressive therapy for severe or refractory cryoglobulinaemic vasculitis with renal involvement; PBS Authority Required for vasculitis indications.
- Plasmapheresis is reserved for life-threatening presentations (rapidly progressive GN, severe skin necrosis, hyperviscosity in Type I).
- Avoid combination interferon + ribavirin regimens; use pangenotypic DAAs which achieve SVR rates >95% and significantly improve renal outcomes.
- Type I cryoglobulinaemia (monoclonal) requires haematology-directed therapy targeting the underlying B-cell or plasma-cell malignancy; management differs substantially from mixed types.
- Monitor cryocrit, complement levels (C4 classically low), HCV RNA, and renal function longitudinally to assess treatment response.
- Aboriginal and Torres Strait Islander peoples have higher HCV prevalence; screen proactively and ensure DAA access in remote communities through telehealth-supported hepatology.
Introduction & Australian Epidemiology
Cryoglobulinaemia is a systemic immune-complex–mediated vasculitis caused by the presence of immunoglobulins (cryoglobulins) that precipitate at temperatures below 37°C and dissolve upon rewarming. When deposited in the renal glomeruli, cryoglobulins cause a characteristic membranoproliferative glomerulonephritis (MPGN) pattern, often leading to progressive chronic kidney disease if the underlying aetiology is not addressed.
In Australia, mixed cryoglobulinaemia (Types II and III) constitutes the vast majority of clinically significant cases, with hepatitis C virus (HCV) identified as the principal driver in 80–90%. Despite the success of Australia's national HCV elimination strategy and widespread access to PBS-subsidised direct-acting antivirals (DAAs) since 2016, cryoglobulinaemic renal disease persists — particularly among individuals with undiagnosed or inadequately treated HCV, and in those with underlying lymphoproliferative or autoimmune disorders.
An estimated 30–50% of patients with chronic HCV infection develop detectable cryoglobulins, though clinically significant cryoglobulinaemic vasculitis occurs in approximately 5–10%. Renal involvement is seen in 20–35% of those with symptomatic mixed cryoglobulinaemia. The introduction of pangenotypic DAAs has markedly improved outcomes, but a subset of patients continue to have active vasculitis and nephritis despite achieving sustained virological response (SVR), necessitating adjunctive immunosuppressive therapy.
Type I cryoglobulinaemia, while less common, is associated with haematological malignancies (multiple myeloma, Waldenström macroglobulinaemia) and carries distinct management priorities, including hyperviscosity syndrome risk and haematology-directed treatment. This guideline addresses the classification, pathophysiology, clinical features, investigation, and management of all cryoglobulinaemia types with emphasis on renal disease, framed within the Australian healthcare context including PBS availability, MBS-funded investigations, and special population considerations.
Classification: Type I, II & III Cryoglobulins
Cryoglobulins are classified by the Brouet system based on the clonality of the immunoglobulin component. Accurate classification is essential as it determines underlying aetiology, clinical features, and therapeutic approach.
| Feature | Type I | Type II (Mixed) | Type III (Mixed) |
|---|---|---|---|
| Immunoglobulin composition | Single monoclonal Ig (IgM, IgG, or IgA) | Monoclonal IgM (rheumatoid factor) + polyclonal IgG | Polyclonal IgM (rheumatoid factor) + polyclonal IgG |
| Proportion of cases | ~10–15% | ~50–60% | ~25–30% |
| Associated conditions | Multiple myeloma, Waldenström macroglobulinaemia, MGUS, CLL | HCV (~80–90%), HBV, HIV, Sjögren syndrome, lymphoma | HCV (~30–50%), autoimmune diseases (SLE, RA), chronic infections |
| Rheumatoid factor | Negative | Strongly positive | Positive (lower titres) |
| Primary mechanism | Hyperviscosity, vascular occlusion | Immune complex deposition, vasculitis | Immune complex deposition, vasculitis |
| Renal disease pattern | Thrombotic microangiopathy, intraglomerular thrombi | MPGN (most common renal pattern) | MPGN, mesangial proliferative GN |
| C4 complement | Normal or mildly low | Markedly low | Low to mildly low |
Subclassification into Type II and III can be difficult as the monoclonal component in Type II may be at low concentration; immunofixation electrophoresis of the dissolved cryoprecipitate is required for accurate typing. In Australia, cryoglobulin testing is performed at major tertiary hospital laboratories and some private reference labs (e.g., Douglass Hanly Moir Pathology, Laverty Pathology). Samples must be collected and transported at 37°C to prevent in-vitro precipitation — coordinate with the laboratory before collection.
Pathophysiology & HCV Association
Mechanisms of Cryoglobulin-Mediated Renal Injury
Cryoglobulins cause renal disease through several interconnected mechanisms:
- Immune complex deposition: Circulating cryoglobulin immune complexes deposit in the subendothelial and mesangial regions of glomerular capillaries, activating the classical complement pathway. This results in C4 consumption and triggers an inflammatory response with infiltration of monocytes and macrophages.
- Membranoproliferative pattern: The histopathological hallmark is MPGN (now classified under the C3GN/immune complex MPGN spectrum in the 2016 ISN/RPS update) with double contours of the glomerular basement membrane on silver stain, subendothelial electron-dense deposits, and occasional intraluminal "thrombi" composed of cryoglobulin deposits with a characteristic amorphous or "fingerprint" ultrastructural appearance on electron microscopy.
- Vasa vasorum vasculitis: Small-vessel vasculitis of the vasa vasorum contributes to ischaemic injury and can cause tubulointerstitial damage in addition to glomerular pathology.
- Type I mechanism: In Type I cryoglobulinaemia, the high concentration of monoclonal protein causes direct vascular occlusion and hyperviscosity rather than classical immune complex-mediated inflammation; the renal lesion is typically thrombotic microangiopathy rather than MPGN.
HCV and Cryoglobulinaemia — The Australian Context
HCV drives mixed cryoglobulinaemia through chronic antigenic stimulation of B lymphocytes. The HCV envelope protein binds CD81 on B cells, promoting clonal expansion — particularly of B cells producing IgM with rheumatoid factor activity. This results in formation of immune complexes (HCV–anti-HCV–IgM-RF) that deposit in vessels and glomeruli.
Australia has an estimated 170,000–200,000 people living with chronic HCV. Since March 2016, unrestricted PBS access to DAAs has transformed outcomes, with over 100,000 Australians treated by 2023. However, cryoglobulinaemic vasculitis can persist or even emerge paradoxically after SVR in a small proportion of patients — likely reflecting ongoing autoreactive B-cell clones no longer suppressed by viral antigen. This phenomenon underscores the importance of continued renal monitoring post-SVR and the role of rituximab in selected patients.
Non-HCV Aetiologies
While HCV dominates, other causes of mixed cryoglobulinaemia encountered in Australian practice include:
- Autoimmune diseases — Sjögren syndrome, systemic lupus erythematosus (SLE), rheumatoid arthritis
- Hepatitis B virus (HBV) — less common than HCV in Australia
- HIV co-infection
- Lymphoproliferative disorders — B-cell non-Hodgkin lymphoma
- Idiopathic — in approximately 5–10% of cases (Type III more often)
Clinical Features (Purpura, Arthralgia, GN)
The clinical spectrum of cryoglobulinaemia ranges from asymptomatic cryoglobulin detection to fulminant systemic vasculitis with multi-organ failure. The classic Meltzer triad — palpable purpura, arthralgia, and weakness — is present in approximately 70–80% of patients with symptomatic mixed cryoglobulinaemia.
Cutaneous Manifestations
- Palpable purpura: The most common presenting feature (seen in ~80%). Typically affects the lower limbs and is exacerbated by cold exposure or prolonged standing. Histology shows leucocytoclastic vasculitis with perivascular IgM and C3 deposition.
- Livedo reticularis: Mottled, net-like violaceous pattern, particularly on the legs.
- Skin ulceration: Chronic, non-healing ulcers particularly over the malleoli; may be severe and refractory.
- Digital ischaemia and gangrene: More common in Type I due to vascular occlusion by high cryoglobulin concentrations.
- Raynaud phenomenon: Present in 30–40% of patients with mixed cryoglobulinaemia.
Musculoskeletal
- Arthralgia: Symmetric, non-erosive polyarthralgia affecting the hands, knees, and ankles. Frank arthritis is uncommon but reported.
- Myalgia: Diffuse muscle pain, often associated with fatigue.
Renal Manifestations
Renal involvement occurs in 20–35% of patients with symptomatic mixed cryoglobulinaemia and is a major determinant of morbidity and mortality. The presentation typically evolves over weeks to months:
Other Organ Involvement
- Peripheral neuropathy: Present in 60–70%. Sensorimotor polyneuropathy or mononeuritis multiplex (e.g., foot drop from peroneal nerve involvement).
- Hepatic: Hepatitis, cirrhosis (directly from HCV rather than cryoglobulinaemia per se).
- Pulmonary: Interstitial lung disease, diffuse alveolar haemorrhage (rare but life-threatening).
- Gastrointestinal: Abdominal pain from mesenteric vasculitis; rarely bowel ischaemia or perforation.
- CNS: Rare; cerebral vasculitis, stroke.
Investigations
Laboratory Investigations
Renal Biopsy
Percutaneous renal biopsy is indicated in patients with suspected cryoglobulinaemic glomerulonephritis (proteinuria, haematuria, declining eGFR) and is the gold standard for diagnosis and prognostication. Key histopathological findings:
- Light microscopy: MPGN pattern with mesangial expansion, endocapillary proliferation, and double contours of GBMs on silver/PAS stain. Intracapillary "thrombi" — large, eosinophilic, amorphous or structured deposits — are characteristic and highly suggestive of cryoglobulinaemic GN when present.
- Immunofluorescence: Granular staining for IgM, IgG, and C3 along capillary walls and in mesangium. IgM often predominates and may show kappa or lambda light chain restriction (Type II).
- Electron microscopy: Subendothelial electron-dense deposits with a distinctive "fingerprint" or annular-tubular substructure representing organised cryoglobulin deposits. This finding is virtually pathognomonic.
Renal biopsy is performed by nephrology at all major Australian tertiary centres. Ultrasound-guided percutaneous biopsy is standard; MBS item 36500 applies.
Additional Investigations
- Renal ultrasound: Assess kidney size, cortical thickness, exclude obstruction. MBS item 55034.
- Nerve conduction studies/EMG: If peripheral neuropathy suspected. MBS item 11000.
- Cryocrit serial monitoring: Quantify cryocrit percentage to track treatment response; correlate with complement and clinical parameters.
- Serum viscosity: If Type I suspected or hyperviscosity symptoms present (visual disturbance, headache, confusion). Not routinely available; tertiary referral.
- Bone marrow biopsy: If haematological malignancy suspected (Type I or refractory Type II); coordinate with haematology.
Management
Management of cryoglobulinaemic renal disease requires a dual approach: (1) treating the underlying cause (most commonly HCV) and (2) controlling the immune-mediated vasculitis when organ-threatening or refractory to antiviral therapy alone. Management should be guided by disease severity, cryoglobulin type, and the presence of life-threatening organ involvement.
Antiviral Therapy — HCV-Associated Cryoglobulinaemia
Direct-acting antivirals (DAAs) are the cornerstone of treatment for HCV-associated mixed cryoglobulinaemia. Eradication of HCV eliminates the chronic antigenic stimulus driving cryoglobulin production and immune complex formation. All patients with HCV-associated cryoglobulinaemia should receive DAA therapy regardless of renal disease severity.
Immunosuppressive Therapy
Immunosuppression is indicated for severe organ-threatening disease, and for patients with persistent vasculitis/nephritis despite SVR. It should be combined with antiviral therapy in HCV-positive patients to prevent viral flare.
Plasmapheresis (Therapeutic Plasma Exchange)
Plasmapheresis physically removes circulating cryoglobulins and is reserved for life-threatening presentations where rapid clearance is required:
- Rapidly progressive glomerulonephritis (RPGN) with deteriorating renal function
- Severe skin necrosis / digital gangrene
- Hyperviscosity syndrome (Type I — this is the primary indication for apheresis in Type I)
- Diffuse alveolar haemorrhage
- Severe neuropathy with motor deficit
Typical regimen: 3–6 exchanges (60 mL/kg per session with 5% albumin replacement) over 1–2 weeks, combined with immunosuppression to suppress new cryoglobulin production. Available at all Australian tertiary centres with apheresis services. MBS item 13700 applies.
Type I Cryoglobulinaemia — Specific Management
Type I cryoglobulinaemia is fundamentally different in pathophysiology and treatment. Management is directed at the underlying haematological malignancy:
- Bortezomib-based regimens for myeloma-associated Type I
- Rituximab ± chemotherapy for Waldenström macroglobulinaemia / B-cell lymphoma
- Plasmapheresis as first-line emergency therapy for hyperviscosity
- Avoid corticosteroids as monotherapy — they do not address the clonal B-cell population
- Haematology co-management is essential
Treatment Algorithm Summary
Monitoring
Longitudinal monitoring is essential to assess treatment response, detect relapse, and manage complications of therapy.
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of hepatitis C infection and its complications, including cryoglobulinaemic renal disease. The AIHW reports that notification rates of HCV in Indigenous Australians are approximately 2–3 times higher than in non-Indigenous Australians, with particularly elevated prevalence in remote and very remote communities. Barriers to care intersect across multiple domains, compounding the risk of late presentation with established cryoglobulinaemic vasculitis and renal impairment.
📚 References
- 1. Muchtar E, Magen H, Gertz MA. How I treat cryoglobulinemia. Blood. 2017;129(3):289–298. doi:10.1182/blood-2016-06-696195.
- 2. Fabrizi F, Plaisier E, Saadoun D, et al. Hepatitis C virus infection, mixed cryoglobulinemia, and kidney disease. Am J Kidney Dis. 2013;61(4):623–637. doi:10.1053/j.ajkd.2012.08.041.
- 3. Roccatello D, Saadoun D, Ramos-Casals M, et al. Cryoglobulinaemia. Nat Rev Dis Primers. 2018;4(1):11. doi:10.1038/s41572-018-0009-4.
- 4. Saadoun D, Resche Rigon M, Pol S, et al. PegIFNα/ribavirin/protease inhibitor combination in hepatitis C virus-associated mixed cryoglobulinemia: results from the French nationwide reference center cohort. Arthritis Rheum. 2013;65(4):1057–1065.
- 5. De Vita S, Quartuccio L, Isola M, et al. A randomized controlled trial of rituximab for the treatment of severe cryoglobulinemic vasculitis. Arthritis Rheum. 2012;64(3):843–853. doi:10.1002/art.34331.
- 6. Australian Government Department of Health. Pharmaceutical Benefits Scheme — Hepatitis C Treatment. Available at: www.pbs.gov.au. Accessed 2024.
- 7. The Kirby Institute. HIV, viral hepatitis and sexually transmissible infections in Australia: Annual Surveillance Report 2023. Sydney: UNSW; 2023.
- 8. Australian Institute of Health and Welfare (AIHW). Aboriginal and Torres Strait Islander Health Performance Framework 2023 — Hepatitis C notifications. Canberra: AIHW; 2023.
- 9. Kidney Health Australia. Chronic Kidney Disease (CKD) Management in Primary Care. 4th ed. Melbourne: Kidney Health Australia; 2020.
- 10. European Association for the Study of the Liver (EASL). EASL Recommendations on Treatment of Hepatitis C: Final Update. J Hepatol. 2020;73(5):1170–1218. doi:10.1016/j.jhep.2020.08.018.
- 11. Brouet JC, Clauvel JP, Danon F, Klein M, Seligmann M. Biologic and clinical significance of cryoglobulins: a report of 86 cases. Am J Med. 1974;57(5):775–788. doi:10.1016/0002-9343(74)90852-3.
- 12. Sethi S, Haas M, Markowitz GS, et al. Mayo Clinic/Renal Pathology Society consensus report on pathologic classification, diagnosis, and reporting of GN. J Am Soc Nephrol. 2016;27(5):1278–1287. doi:10.1681/ASN.2015060612.
- 13. RHDAustralia (ARF/RHD Register). Guidelines for Acute Rheumatic Fever and Rheumatic Heart Disease in Australia. Darwin: Menzies School of Health Research; 2020.
- 14. Royal Australian College of General Practitioners (RACGP). Australian Immunisation Handbook — Immunisation of individuals with altered immunocompetence. Available at: immunisationhandbook.health.gov.au. Accessed 2024.