📋 Key Information Summary
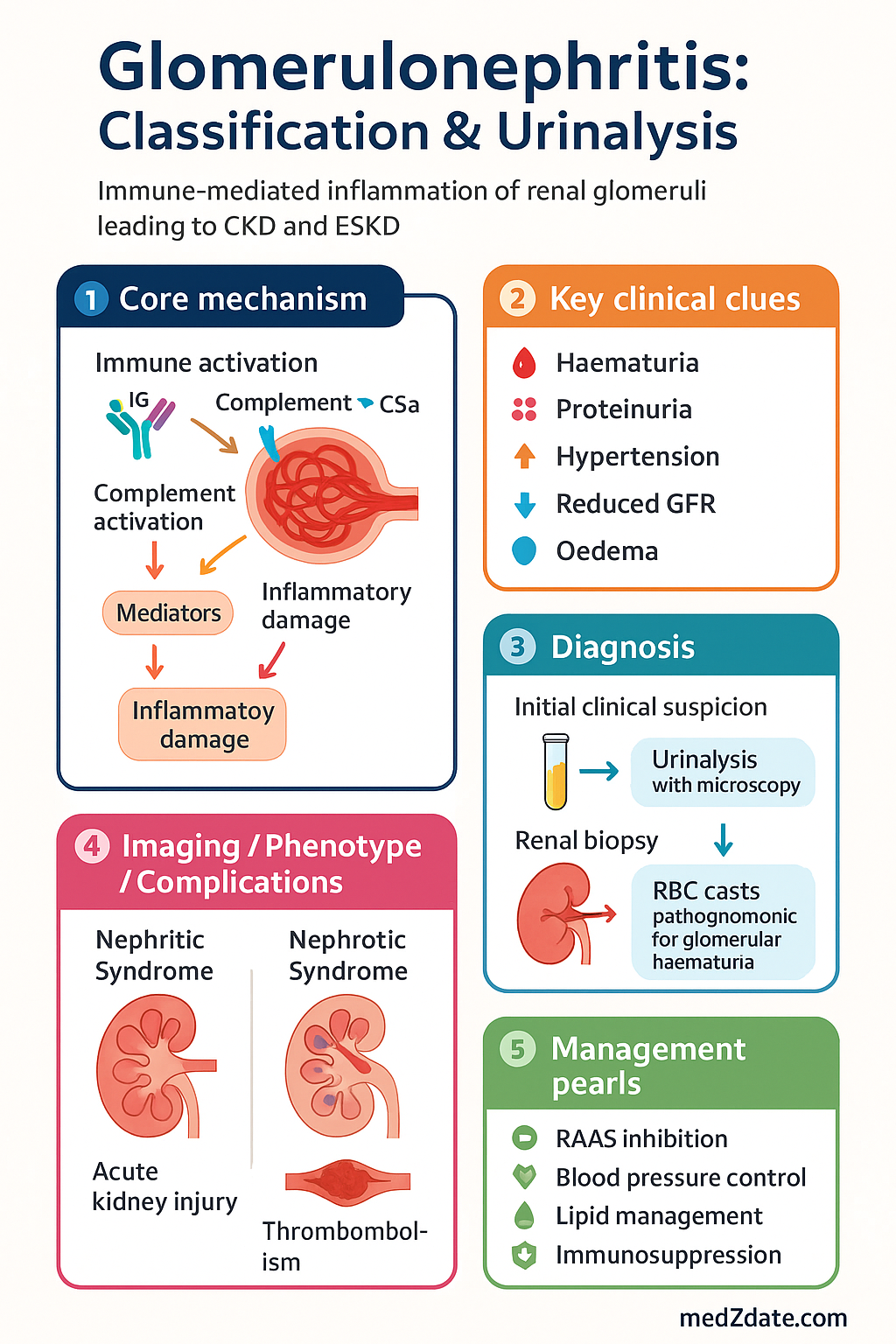
- Glomerulonephritis (GN) is an immune-mediated inflammation of the renal glomeruli, a leading cause of chronic kidney disease (CKD) and end-stage kidney disease (ESKD) in Australia.
- The two primary clinical syndromes are nephritic syndrome (haematuria, hypertension, reduced GFR) and nephrotic syndrome (heavy proteinuria, hypoalbuminaemia, oedema).
- Urinalysis with microscopy is the cornerstone of initial assessment; dysmorphic red blood cells (RBCs) and RBC casts are pathognomonic for glomerular haematuria.
- A renal biopsy is required for definitive histological classification and to guide specific immunosuppressive therapy in most forms of progressive GN.
- Primary GN includes IgA nephropathy, minimal change disease, focal segmental glomerulosclerosis (FSGS), membranous nephropathy, and membranoproliferative GN.
- Secondary GN causes include lupus nephritis, anti-GBM disease, ANCA-associated vasculitis, diabetic nephropathy, and infection-related GN (e.g., post-streptococcal).
- Management requires a dual approach: supportive care (RAAS inhibition, blood pressure, and lipid control) and disease-specific immunosuppression.
- Key investigations include serum complement (C3, C4), anti-nuclear antibody (ANA), anti-dsDNA, ANCA, anti-GBM antibodies, serum/urine protein electrophoresis, and hepatitis B/C and HIV serology.
- Refer urgently to a nephrologist for nephrotic syndrome, rapidly progressive glomerulonephritis (RPGN), or a sustained fall in eGFR >25%.
- Aboriginal and Torres Strait Islander peoples experience a higher burden of GN and CKD, often with later presentation and more rapid progression, requiring culturally safe care and early referral.
Introduction & Australian Epidemiology
Glomerulonephritis (GN) encompasses a group of immune-mediated diseases characterised by inflammation of the glomeruli, the kidney's filtering units. It is a major cause of chronic kidney disease (CKD), kidney failure, and premature cardiovascular morbidity in Australia. The clinical presentation is often insidious, detected through abnormalities in urinalysis—specifically proteinuria and haematuria—or a decline in estimated glomerular filtration rate (eGFR).
In Australia, GN accounts for approximately 10-15% of people commencing kidney replacement therapy (dialysis or transplant). IgA nephropathy is the most common primary GN, while lupus nephritis and ANCA-associated vasculitis are significant secondary causes. The epidemiology varies with demographics; for instance, IgA nephropathy is more common in young adults, while membranous nephropathy peaks in middle-aged males.
Early and accurate classification via clinical syndrome assessment, serological testing, and histological examination is critical, as treatment pathways differ radically. This guideline provides an evidence-based framework for the classification, investigation, and initial management of GN within the Australian healthcare context.
Nephritic vs Nephrotic Syndrome
The initial clinical presentation of GN is typically categorised into two overlapping but distinct syndromes, which guide the urgency and direction of investigation.
| Feature | Nephritic Syndrome | Nephrotic Syndrome |
|---|---|---|
| Primary Defect | Inflammation & reduced glomerular filtration. | Increased glomerular permeability to protein. |
| Urinalysis | Haematuria (microscopic or macroscopic), often with RBC casts. Proteinuria typically sub-nephrotic (<3.5 g/day). | Heavy proteinuria (≥3.5 g/day), oval fat bodies, fatty casts. Haematuria may be absent. |
| Key Features | Hypertension, reduced eGFR, oliguria, oedema (often mild). | Generalised oedema/anasarca, hypoalbuminaemia (<25 g/L), hyperlipidaemia, frothy urine. |
| Complications | Acute kidney injury (AKI), fluid overload. | Thromboembolism (DVT/PE), infection risk, malnutrition, accelerated atherosclerosis. |
| Typical Primary GN | IgA Nephropathy (common), Post-infectious GN, Crescentic GN. | Minimal Change Disease, FSGS, Membranous Nephropathy. |
Urinalysis Interpretation & Casts
Urinalysis with phase-contrast microscopy of a fresh, mid-stream urine specimen is the single most important non-invasive test in GN.
Key Components
- Dipstick: Positive for blood (haematuria) and protein. A protein:creatinine ratio (PCR) or albumin:creatinine ratio (ACR) on a spot urine quantifies proteinuria.
- Microscopy - Red Cells: Dysmorphic RBCs (variable size, shape, blebs) indicate a glomerular origin. Isomorphic RBCs suggest a non-glomerular (urological) source.
- Casts: Formed in the renal tubules and reflect the underlying pathology.
Glomerular Biopsy: Indications & Interpretation
A percutaneous renal biopsy is the gold standard for diagnosing the specific type of GN. It is performed under real-time ultrasound guidance by a nephrologist or interventional radiologist.
Common Indications for Biopsy in Suspected GN
- Nephrotic syndrome in adults.
- Unexplained nephritic syndrome or persistent glomerular haematuria with proteinuria.
- Rapidly progressive glomerulonephritis (RPGN) - urgent biopsy required.
- Acute kidney injury (AKI) in the context of active urinary sediment.
- Systemic disease (e.g., SLE, vasculitis) with evidence of renal involvement.
Interpretation: The Three Compartments
The biopsy is examined by light microscopy (LM), immunofluorescence (IF), and electron microscopy (EM).
| Technique | Key Findings | Classifies |
|---|---|---|
| Light Microscopy | Cellularity, sclerosis, crescents, thickening of GBM, inflammatory infiltrate. | Pattern (e.g., diffuse, focal) and activity/chronicity. |
| Immunofluorescence | Deposits of IgG, IgA, IgM, C3, C1q. Pattern (granular, linear). | Aetiology (e.g., IgA-dominant = IgA Nephropathy; C3-dominant = C3 glomerulopathy). |
| Electron Microscopy | Location of deposits (subepithelial, subendothelial, mesangial), podocyte foot process effacement. | Specific disease (e.g., subepithelial "humps" in post-infectious GN; diffuse foot process effacement in Minimal Change). |
Classification of GN (Primary vs Secondary)
Accurate classification integrates clinical, serological, and histological data to separate primary (idiopathic) GN from GN secondary to systemic disease, infection, or drugs.
Primary Glomerulonephritis
The disease process is confined to the kidney. Diagnosis relies heavily on biopsy.
Secondary Glomerulonephritis
GN is part of a systemic disorder. Identifying the underlying cause is paramount.
| Underlying Condition | Typical GN Pattern | Key Diagnostic Clues |
|---|---|---|
| Systemic Lupus Erythematosus (SLE) | Lupus Nephritis (ISN/RPS Class I-VI) | Positive ANA, anti-dsDNA, low complement. Biopsy shows "full-house" IF (IgG, IgM, IgA, C3, C1q). |
| Diabetes Mellitus | Diabetic Nephropathy | Long-standing diabetes, retinopathy, nodular glomerulosclerosis (Kimmelstiel-Wilson). |
| Anti-GBM Disease | Crescentic GN (Type I) | Pulmonary-renal syndrome (haemoptysis, haematuria). Linear IgG on IF. Serum anti-GBM Ab positive. |
| Infection (e.g., HCV, HBV, Strep) | MPGN, Membranous | Positive serology. Subendothelial deposits (HCV), subepithelial "humps" (post-strep). |
Aboriginal and Torres Strait Islander Health
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of kidney disease, including GN, often at a younger age and with more rapid progression to kidney failure.
📚 References
- 1. Kidney Health Australia. Chronic Kidney Disease (CKD) Management in Primary Care. 4th edition. 2020.
- 2. KDIGO. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney Int. 2021;100(4):S1-S276.
- 3. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. Cat. no. CKD 7. Canberra: AIHW; 2023.
- 4. Rangan GK, Tchan MC, Tong A, et al. Recent advances in lupus nephritis. Nephrology. 2021;26(10):773-786.
- 5. Roberts DM, Jones RN, Dwyer KM, et al. The Australian and New Zealand vasculitis society (ANZVas) guidelines for the management of ANCA-associated vasculitis. Intern Med J. 2023;53(6):862-878.
- 6. Gracey M, King M. Indigenous health part 1: determinants and disease patterns. Lancet. 2009;374(9683):65-75.
- 7. Floege J, Barbour SJ, Cattran DC, et al. Management and treatment of glomerular diseases (part 1): conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019;95(2):268-280.
- 8. The Royal Australian College of General Practitioners (RACGP). Urinalysis in general practice. 2022.
- 9. Hughes PD, Cohney SJ, Kanh KY, et al. The CARI guidelines: indicators for renal biopsy in adults with glomerulonephritis. Nephrology. 2012;17(Suppl 1):S1-S42.
- 10. Tong A, Howell M, Wong G, et al. The perspectives of adults with glomerulonephritis on clinical trial design and research participation. Kidney Int Rep. 2020;5(8):1241-1251.