📋 Key Information Summary
- Urinalysis with dipstick and microscopy is the single most cost-effective nephrology investigation available in primary care and emergency medicine in Australia.
- Midstream urine (MSU) collection with prompt refrigeration or boric acid preservation is essential to minimise false-positive culture and morphological artefact.
- Dipstick haematuria (≥1+ / ≥10 RBC/µL) requires confirmation on microscopy; false positives occur with myoglobinuria, alkaline urine & menstrual contamination.
- Dipstick protein (≥1+) should always be quantified using albumin-to-creatinine ratio (ACR) on a spot urine — ACR is MBS-rebated in Australia and replaces 24-hour collections in most settings.
- ACR >3.5 mg/mmol (women) or >2.5 mg/mmol (men) on two of three samples over ≥3 months defines persistent albuminuria (KDIGO stage A2–A3).
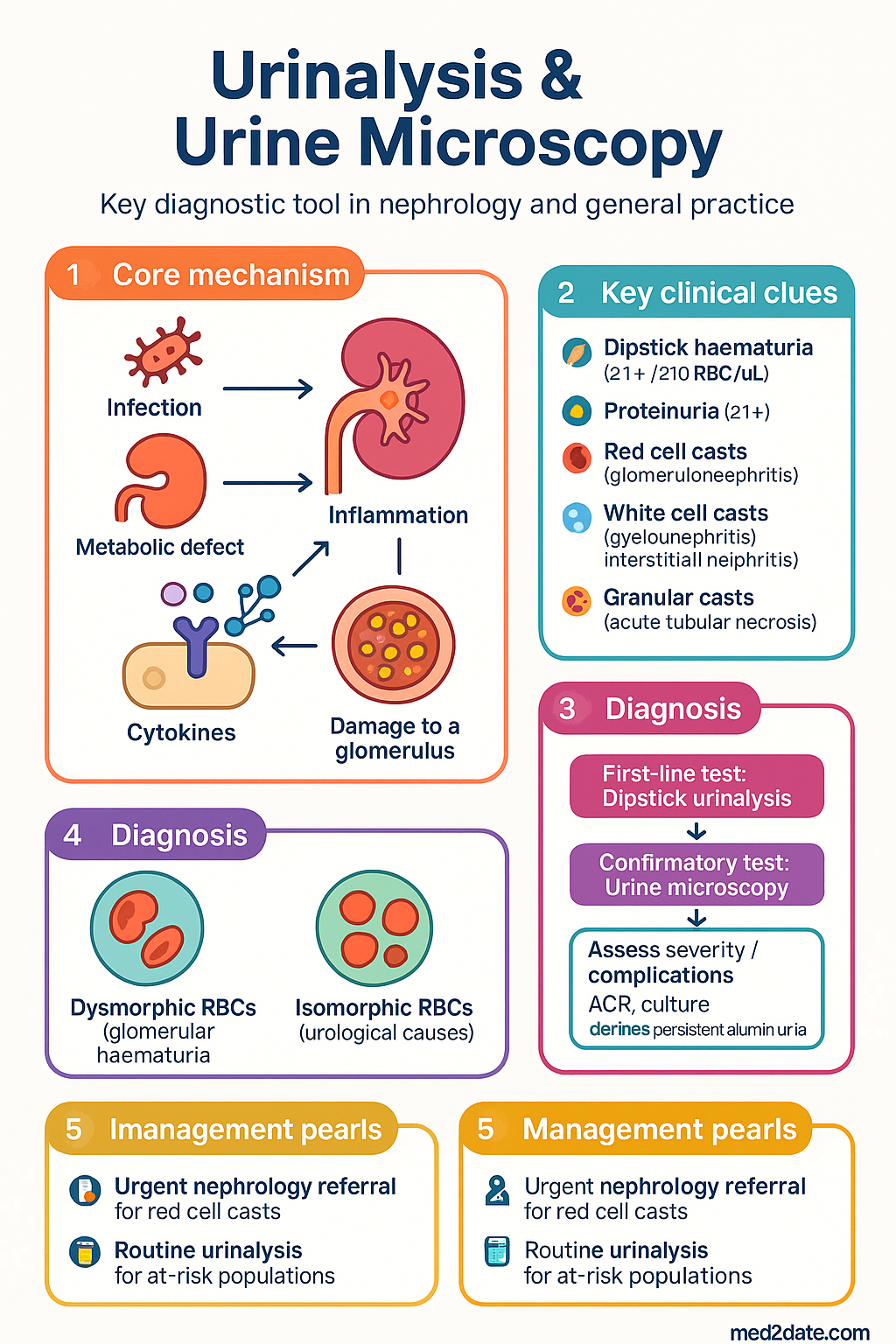
- Red cell casts are pathognomonic for glomerulonephritis — their presence mandates urgent nephrology referral.
- White cell casts suggest pyelonephritis or acute interstitial nephritis; WBC casts with eosinophiluria points toward drug-induced interstitial nephritis.
- Granular ("muddy brown") casts are the hallmark of acute tubular necrosis (ATN).
- Dysmorphic RBCs (acanthocytes) with >5% on phase-contrast microscopy indicate a glomerular source of haematuria; isomorphic RBCs suggest urological causes.
- WBC esterase and nitrite on dipstick have high specificity for UTI but limited sensitivity; microscopy and culture remain the gold standard.
- Glycosuria in the absence of hyperglycaemia suggests proximal tubular dysfunction (Fanconi syndrome) rather than diabetes.
- Aboriginal and Torres Strait Islander peoples experience significantly higher rates of CKD and glomerulonephritis; routine urinalysis should be incorporated into annual health checks under MBS Item 715.
Introduction & Australian Epidemiology
Urinalysis with urine microscopy is an indispensable investigation in nephrology and general practice. It provides rapid, inexpensive, and clinically rich information about renal parenchymal disease, urinary tract infection, systemic disorders, and metabolic derangements. The urine dipstick serves as a sensitive screening tool, while microscopy of a freshly centrifuged specimen provides diagnostic specificity — identifying cellular elements, casts, and crystals that delineate the site and nature of renal pathology.
In Australia, chronic kidney disease (CKD) affects approximately 1 in 10 adults, with over 1.7 million Australians estimated to have indicators of kidney disease (AIHW 2023). Aboriginal and Torres Strait Islander peoples experience end-stage kidney disease at rates 6–8 times higher than non-Indigenous Australians, and glomerulonephritis remains a disproportionately common cause in this population. Dipstick urinalysis is a core component of the MBS Item 715 Aboriginal and Torres Strait Islander health check and is recommended annually for at-risk populations.
The combination of dipstick urinalysis and urine microscopy allows clinicians to distinguish glomerular from non-glomerular haematuria, to identify the nephrotic spectrum (proteinuria), to detect infection, and to recognise tubular injury patterns — often before serum creatinine rises. Red cell casts indicate glomerulonephritis, white cell casts suggest pyelonephritis or interstitial nephritis, and granular ("muddy brown") casts indicate acute tubular necrosis (ATN). Understanding these findings is fundamental to appropriate triage, investigation, and referral in Australian clinical practice.
Specimen Collection & Processing
Accurate urinalysis depends on correct specimen collection, handling, and processing. In Australian practice, the midstream urine (MSU) specimen remains the standard for both dipstick and microscopy.
Collection Method
- Midstream urine (MSU): Clean-catch, midstream specimen after retracting the foreskin or cleansing the vulva. Discard the initial stream to minimise urethral flora contamination.
- Catheter specimen: Aspirate from the catheter port (not the drainage bag) using aseptic technique.
- Suprapubic aspiration: Gold standard for neonatal specimens; eliminates contamination risk entirely.
- First morning specimen: Preferred for ACR quantification and pregnancy screening — most concentrated and most comparable between samples.
Handling & Timing
For urine microscopy specifically, the specimen should be fresh, at room temperature, and analysed by an experienced scientist or clinician. Refrigerated specimens may show precipitation of amorphous urates or phosphates, which should not be confused with pathological crystals.
Dipstick Interpretation
The urine dipstick (e.g., Siemens Multistix®, Roche Combur-Test®) provides a rapid semi-quantitative assessment of multiple analytes. Each pad reacts via a specific chemical mechanism, and clinicians must understand both the capabilities and limitations of each test.
pH
Normal urine pH ranges from 4.5–8.0. Persistent alkaluria (pH >7.0) may suggest infection with urease-producing organisms (e.g., Proteus mirabilis) or renal tubular acidosis (RTA) Type 1 (distal). Acidic urine (pH <5.0) is seen with metabolic acidosis, high-protein diets, and uric acid stone formers.
Specific Gravity (SG)
Normal range 1.001–1.035. Low SG (<1.010) may indicate impaired concentrating ability (interstitial nephritis, CKD, diabetes insipidus). High SG (>1.030) suggests dehydration or glycosuria. The dipstick SG is based on ionic concentration and can be falsely elevated by glucose, protein, or intravenous contrast agents.
Protein
| Dipstick result | Approximate concentration | Action |
|---|---|---|
| Negative | <150 mg/L (<0.15 g/L) | No further action if low risk |
| Trace | 150–300 mg/L | Repeat; quantify with ACR if persistent |
| 1+ | 300 mg/L (~0.3 g/L) | Quantify with spot ACR (MBS-rebated) |
| 2+ | 1000 mg/L (~1.0 g/L) | Quantify with ACR; consider nephrotic-range workup |
| 3+ | 3000 mg/L (~3.0 g/L) | Nephrology referral; quantify urgently |
| 4+ | >5000 mg/L (>5.0 g/L) | Urgent nephrology — likely nephrotic syndrome |
The dipstick pad is most sensitive to albumin and has poor sensitivity for Bence Jones proteins (light chains), Tamm-Horsfall protein, or beta-2 microglobulin. In suspected myeloma, always request urine protein electrophoresis (UPEP) and serum free light chain assay.
Blood (Haemoglobin / Myoglobin)
The blood pad detects free haemoglobin and myoglobin via the peroxidase-like activity of the haem moiety. It does NOT detect intact RBCs directly — rather, it detects haem released from lysed red cells.
| Dipstick result | Approximate RBC count | Interpretation |
|---|---|---|
| Negative | <10 RBC/µL | Normal |
| Trace / Non-haemolysed | 10–25 RBC/µL | Confirm on microscopy |
| 1+ / Small | 25–50 RBC/µL | Microscopic haematuria; assess morphology |
| 2+ / Moderate | 50–200 RBC/µL | Investigate: glomerular vs non-glomerular |
| 3+ / Large | >200 RBC/µL | Significant haematuria; urgent evaluation |
| Trace intact / Intact RBCs only | Variable | Few intact RBCs, no free Hb; may be artefactual |
Leucocyte Esterase (WBC)
Leucocyte esterase is an enzyme produced by neutrophils and, to a lesser extent, macrophages. A positive result suggests pyuria (>10 WBC/µL) and may indicate urinary tract infection, interstitial nephritis, or other inflammatory conditions.
| Result | Approximate WBC count | Clinical action |
|---|---|---|
| Negative | <10 WBC/µL | UTI unlikely (NPV ~95%) |
| Trace | 10–25 WBC/µL | Borderline; send for microscopy + culture if symptomatic |
| Small (1+) | 25–75 WBC/µL | Send MSU for M+C |
| Moderate (2+) | 75–500 WBC/µL | Send MSU; consider empirical antibiotics if symptomatic |
| Large (3+) | >500 WBC/µL | High likelihood of UTI; treat empirically per eTG |
Nitrite
Many Gram-negative bacteria (e.g., E. coli, Klebsiella, Proteus) convert urinary nitrate to nitrite. A positive nitrite test has high specificity (~95%) for bacteriuria but poor sensitivity (~45–60%) because:
- Gram-positive organisms (Enterococcus, Staphylococcus saprophyticus) do not reduce nitrate.
- Urine must remain in the bladder ≥4 hours for sufficient nitrate conversion (first morning specimen preferred).
- Low dietary nitrate intake or diuresis reduces substrate availability.
Combined leucocyte esterase + nitrite: If both are positive, the positive predictive value for UTI exceeds 95% in symptomatic patients. If both are negative, UTI is unlikely (NPV >95%) and microscopy/culture may be deferred unless the patient is immunocompromised, pregnant, or has a complicated presentation.
Glucose
The dipstick glucose pad uses glucose oxidase to detect glycosuria. Normally, all filtered glucose is reabsorbed by SGLT2 transporters in the proximal tubule; glycosuria appears when the renal threshold (~10 mmol/L) is exceeded.
| Scenario | Interpretation |
|---|---|
| Glycosuria with hyperglycaemia | Diabetes mellitus — confirm with HbA1c or fasting glucose |
| Glycosuria with normoglycaemia | Renal glycosuria (benign) or proximal tubular dysfunction (Fanconi syndrome) |
| SGLT2 inhibitor use | Expected — dapagliflozin (Forxiga®), empagliflozin (Jardiance®) inhibit SGLT2 |
| Glycosuria in pregnancy | Lowered renal threshold in pregnancy; may be physiological but screen for GDM |
Ketones
The dipstick detects acetoacetate (and, to a lesser extent, acetone) but does NOT detect beta-hydroxybutyrate, which is the predominant ketone in diabetic ketoacidosis (DKA). Positive ketones on dipstick may be seen in starvation, prolonged fasting, low-carbohydrate diets, DKA (late), and alcoholic ketoacidosis. In established DKA, serum beta-hydroxybutyrate (MBS-rebated) is a superior marker for monitoring.
Bilirubin & Urobilinogen
Conjugated bilirubin in urine (positive dipstick) suggests hepatobiliary disease (obstructive jaundice, hepatitis). Unconjugated bilirubin is not water-soluble and does not appear in urine. Elevated urobilinogen suggests haemolytic anaemia or hepatocellular disease. Absent urobilinogen with positive bilirubin suggests complete biliary obstruction.
Urine Microscopy: Casts, Cells & Crystals
Urine microscopy is the definitive step in urinalysis. A standardised examination of a centrifuged specimen (10–15 mL at 1500–2000 rpm for 5 minutes, resuspend the sediment in 0.5–1 mL of supernatant) under high-power field (×400) provides diagnostic information unavailable from the dipstick alone.
Phase-contrast microscopy is preferred for RBC morphology assessment but may not be available in all Australian laboratories; bright-field microscopy remains acceptable for cast and crystal identification.
Casts
Urinary casts are cylindrical structures formed within the renal tubular lumen from Tamm-Horsfall mucoprotein (uromodulin). They reflect the conditions of the tubular microenvironment at the time of their formation. All casts have a characteristic parallel-sided, rounded-end morphology.
| Cast type | Appearance | Clinical significance |
|---|---|---|
| Hyaline casts | Transparent, low refractive index; visible only under reduced light | Normal finding (<2/LPF); increased with exercise, dehydration, CKD. Non-specific. |
| RBC casts | Reddish-brown; contain entrapped RBCs within the cast matrix | Pathognomonic of glomerulonephritis (IgA nephropathy, lupus nephritis, ANCA vasculitis, anti-GBM disease). Urgent nephrology referral. |
| WBC casts | Granular, contain intact or degenerating neutrophils | Pyelonephritis, acute interstitial nephritis (drug-induced), lupus nephritis. Distinguish from WBC clumps (non-cast). |
| Granular casts | Coarse or fine granules; "muddy brown" appearance in ATN | Hallmark of acute tubular necrosis (ATN). Also seen in CKD, GN. Coarse > fine = more severe tubular injury. |
| Muddy brown casts | Dark brown, coarsely granular; contain tubular epithelial cell debris | Highly specific for ischaemic or nephrotoxic ATN (contrast nephropathy, aminoglycosides, rhabdomyolysis). |
| Waxy casts | Highly refractile, sharp broken edges, homogeneous | Chronic kidney disease, advanced tubular atrophy. Indicates longstanding renal parenchymal disease. |
| Fatty casts | Contain refractile lipid droplets (Maltese cross under polarised light) | Nephrotic syndrome (lipiduria). Seen with oval fat bodies. |
| TEC casts | Contain tubular epithelial cells | Acute tubular necrosis, toxic nephropathy (e.g., ethylene glycol), interstitial nephritis. |
| Pigmented casts | Brown (myoglobin) or red-brown (haemoglobin) | Rhabdomyolysis (myoglobin), haemolysis (haemoglobin). |
Cells
| Cell type | Findings | Significance |
|---|---|---|
| Red blood cells | >2 RBC/HPF is abnormal (>2000/mL) | Haematuria — assess morphology (see below) |
| Dysmorphic RBCs | Irregular membrane: acanthocytes (ring forms with blebs), fragmented RBCs | Glomerular origin — passage through damaged GBM causes distortion |
| Isomorphic RBCs | Uniform, round, biconcave — normal morphology | Non-glomerular source: urothelial, calculi, tumour, BPH |
| White blood cells | >5 WBC/HPF is abnormal (pyuria) | UTI, interstitial nephritis, prostatitis, TB, interstitial cystitis |
| Eosinophils | Hansel's stain or Wright's stain >1% of urinary WBCs | Drug-induced interstitial nephritis (PPIs, NSAIDs, antibiotics), cholesterol atheroemboli |
| Tubular epithelial cells (TECs) | Large, round, single nucleus; may be vacuolated | ATN, toxic nephropathy, rejection (transplant). >5/HPF is significant. |
| Squamous cells | Large, flat, irregular; with nucleus | Contamination from external genitalia. If abundant, repeat MSU collection. |
| Oval fat bodies | TECs containing lipid droplets; Maltese cross under polarised light | Nephrotic syndrome (lipiduria) |
Bacteria & Yeasts
Bacteria visible on unspun urine microscopy suggest >10⁵ CFU/mL. However, bacteria should always be confirmed by culture (MBS-rebated midstream urine culture with antimicrobial susceptibility). Yeast forms (oval budding cells, pseudohyphae) suggest Candida species — particularly in catheterised patients, diabetics, and immunocompromised hosts.
Crystals
| Crystal type | pH preference | Appearance | Significance |
|---|---|---|---|
| Calcium oxalate | Any pH | Envelope (dihydrate) or dumbbell/biconcave (monohydrate) | Normal in small numbers. Large quantities: ethylene glycol poisoning, hyperoxaluria, Crohn's disease, jejunoileal bypass. |
| Uric acid | Acidic (<5.5) | Rhomboid, rosette, or barrel-shaped; yellow-brown | Often benign (concentrated acidic urine). Associated with gout, tumour lysis syndrome. Precursor to uric acid stones. |
| Struvite (triple phosphate) | Alkaline (>7.0) | "Coffin-lid" rectangular prisms | Urease-producing bacteria (Proteus); associated with staghorn calculi. |
| Calcium phosphate | Alkaline (>6.5) | Needle-shaped or rosette; colourless | Seen in alkaline urine; may be associated with RTA Type 2 or hyperparathyroidism. |
| Cystine | Acidic | Flat hexagonal plates with well-defined edges | Pathognomonic of cystinuria (autosomal recessive). Confirm with urine cystine quantification. |
| Amorphous urates | Acidic | Granular, yellow-brown; dissolve on warming | Non-pathological; artefact of refrigeration. |
| Amorphous phosphates | Alkaline | Granular, colourless; dissolve with acetic acid | Non-pathological; artefact of refrigeration. |
| Drug crystals | Variable | Variable morphology (e.g., aciclovir — fine needles; sulfonamides — characteristic shapes; indinavir — star-burst) | Obstructive AKI possible with aciclovir, sulfonamides, methotrexate. |
Proteinuria: Quantification
Persistent proteinuria is both a marker and a driver of progressive kidney disease. Quantification is essential after a positive dipstick to stratify risk, guide investigation, and monitor treatment response.
Quantification Methods
| Method | Specimen | Normal values | MBS item | Advantages |
|---|---|---|---|---|
| Albumin-to-Creatinine Ratio (ACR) | Random spot urine (first morning preferred) | <2.5 mg/mmol (♂) <3.5 mg/mmol (♀) | MBS 69414 | Single sample; corrects for concentration; most sensitive for early albuminuria (diabetic nephropathy, hypertensive nephrosclerosis) |
| Protein-to-Creatinine Ratio (PCR) | Random spot urine | <15 mg/mmol | MBS 69414 | Correlates well with 24-hr total protein; includes all proteins (not just albumin); useful when glomerular protein loss is the primary concern |
| 24-hour urine protein | Timed 24-hour collection | <150 mg/24hr | MBS 69410 (quantitative urine protein) | Traditional gold standard; cumbersome, error-prone collection; now largely replaced by ACR/PCR in Australia |
| Urine dipstick protein | Random urine | Negative (<150 mg/L) | N/A (point-of-care) | Screening only; must be quantified if positive |
KDIGO Classification of Albuminuria
ACR vs PCR: When to Use Which?
ACR is the preferred first-line test in Australia for screening and monitoring of CKD (KDIGO, RACGP, Kidney Health Australia). It is more sensitive for detecting early nephropathy because albumin is the first protein to leak through a damaged glomerular barrier.
PCR is useful when total protein loss needs assessment — for example, in suspected nephrotic syndrome (PCR >500 mg/mmol, equivalent to >3.5 g/day) or when non-albumin proteins (e.g., light chains in myeloma) may be contributing. In practice, a PCR >100 mg/mmol roughly corresponds to >1 g/day of proteinuria.
Causes of Non-Glomerular Proteinuria
- Tubular: Low-molecular-weight proteins (beta-2 microglobulin, alpha-1 microglobulin) — ATN, interstitial nephritis, Fanconi syndrome. PCR usually <100 mg/mmol.
- Overflow: Excess circulating proteins filtered beyond tubular reabsorption capacity — myeloma (Bence Jones / free light chains), rhabdomyolysis (myoglobin), haemolysis (haemoglobin).
- Post-renal: Tamm-Horsfall protein, inflammatory exudate from lower urinary tract — UTI, prostatitis, malignancy.
Haematuria: Glomerular vs Non-Glomerular
Haematuria — the presence of blood in the urine — is a common finding in primary care and emergency medicine. Distinguishing glomerular from non-glomerular haematuria is the critical initial diagnostic step, as it determines the subsequent investigation pathway and urgency of referral.
Definitions
- Microscopic haematuria: ≥3 RBC/HPF on centrifuged specimen (or ≥10 RBC/µL on automated urinalysis); dipstick 1+ to 2+. Patient appears to have clear urine.
- Macroscopic (frank) haematuria: Visible blood in urine — from cola-coloured to frankly red. Always pathological and warrants investigation.
- Persistent microscopic haematuria: Haematuria on ≥2 of 3 specimens over ≥3 months, in the absence of transient causes.
Distinguishing Glomerular from Non-Glomerular Haematuria
| Feature | Glomerular | Non-Glomerular |
|---|---|---|
| Urine colour | Cola / smoky / brown | Pink / red / frankly bloody |
| RBC morphology | Dysmorphic (>5% acanthocytes on phase-contrast) | Isomorphic (uniform, biconcave) |
| RBC casts | Present (pathognomonic) | Absent |
| Proteinuria | Often significant (ACR >30 mg/mmol or PCR >100 mg/mmol) | Minimal or absent (<1+ on dipstick) |
| Associated symptoms | Oedema, hypertension, oliguria | Dysuria, frequency, flank pain, clots |
| Clinical context | Young adult, recent URTI, rash (Henoch-Schönlein), joint pain (SLE), sinusitis (GPA) | Age >40, smoker, occupational exposures, BPH, recent catheterisation |
| Common aetiologies | IgA nephropathy, lupus nephritis, Alport syndrome, anti-GBM, ANCA vasculitis | UTI, urolithiasis, urothelial carcinoma, BPH, exercise-induced, trauma |
| Investigation pathway | Nephrology referral → serology → renal biopsy | Urology referral → imaging (US, CT KUB) → cystoscopy |
Investigation Algorithm
Urgent Referral Criteria (Nephrology)
- Macroscopic haematuria with red cell casts
- Microscopic haematuria + proteinuria ACR >30 mg/mmol
- Rapidly declining eGFR (>25% fall in 3 months, or >15 mL/min/year decline)
- Suspected vasculitis: haematuria + constitutional symptoms + purpura / sinusitis / mononeuritis multiplex
- Anti-GBM disease: haemoptysis + haematuria (Goodpasture syndrome)
- Nephrotic syndrome: oedema + albuminuria ACR >220 mg/mmol + hypoalbuminaemia