📋 Key Information Summary
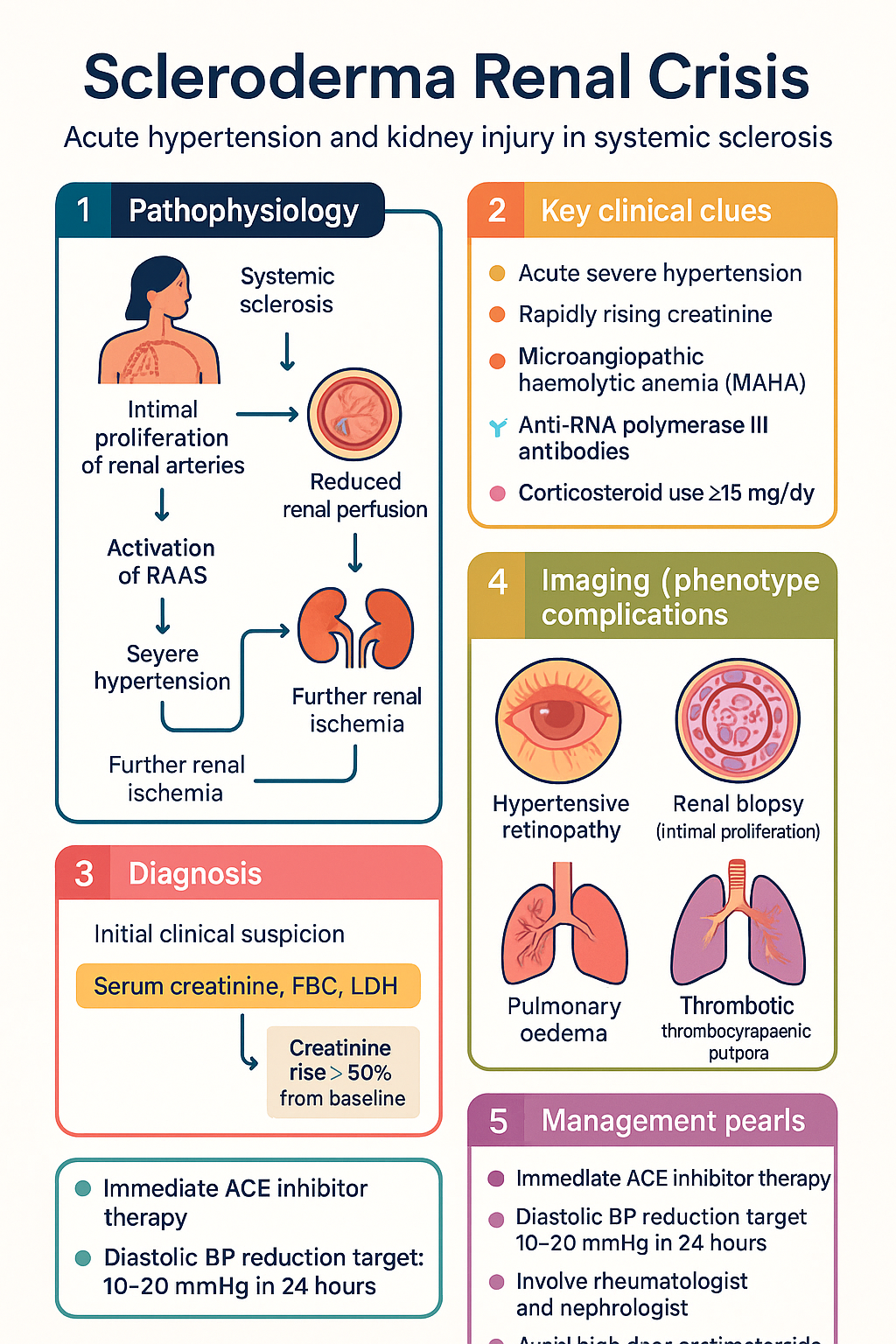
- Scleroderma renal crisis (SRC) is a medical emergency characterised by acute severe hypertension and rapidly progressive acute kidney injury (AKI) in patients with systemic sclerosis (SSc).
- SRC occurs predominantly in diffuse cutaneous SSc (dcSSc), typically within the first 3–5 years of disease onset.
- Anti-RNA polymerase III antibodies are the strongest serological risk factor (present in ~40–60% of SRC cases); anti-centromere antibodies are protective.
- Corticosteroids ≥15 mg/day prednisolone equivalent increase SRC risk — use the lowest effective dose in early dcSSc.
- ACE inhibitors (enalapril, ramipril) are first-line therapy and have dramatically reduced mortality from >80% to ~10–20%.
- Start ACE inhibitors immediately upon clinical suspicion — do not wait for full investigation results.
- Aim for a diastolic BP reduction of 10–20 mmHg within the first 24 hours and gradual normalisation over 48–72 hours.
- Do not discontinue ACE inhibitors even if dialysis is required — renal recovery can occur weeks to months later.
- Approximately 50–70% of patients will require dialysis acutely; ~40–55% of these will eventually discontinue dialysis with continued ACE inhibitor therapy.
- Thrombotic microangiopathy (TMA) with microangiopathic haemolytic anaemia (MAHA) may occur and can mimic thrombotic thrombocytopaenic purpura (TTP).
- Involvement of a rheumatologist and nephrologist is essential; consider transfer to a renal/transplant centre for severe cases.
- ATSI patients may have delayed presentation due to geographic isolation — early rheumatology follow-up and GP education are critical in remote communities.
Introduction & Australian Epidemiology
Scleroderma renal crisis (SRC) is an acute, life-threatening complication of systemic sclerosis (SSc) characterised by the abrupt onset of severe hypertension, rapidly progressive acute kidney injury (AKI), and often microangiopathic haemolytic anaemia (MAHA). It is one of the most feared visceral manifestations of SSc and, prior to the introduction of ACE inhibitors, carried a mortality exceeding 80%. Even in the current era, in-hospital mortality remains approximately 10–20%, with significant long-term morbidity.
In Australia, the estimated prevalence of SSc is approximately 20–40 per 100,000 population, with SRC affecting 2–15% of patients with SSc, depending on the subset. Diffuse cutaneous SSc (dcSSc) carries the highest risk, with an estimated 10–20% of dcSSc patients developing SRC within the first 5 years of disease. The Australian Scleroderma Cohort Study and published data from tertiary centres in Melbourne, Sydney, and Perth have contributed significantly to the understanding of SRC risk factors, serological associations, and outcomes in the Australian context.
Aboriginal and Torres Strait Islander Australians appear to have a higher prevalence of autoimmune connective tissue diseases, although specific SRC incidence data in ATSI populations remain limited. Geographic barriers to specialist care in remote and very remote areas may delay recognition and initiation of life-saving ACE inhibitor therapy.
Pathophysiology & Risk Factors
Pathophysiology
SRC results from a distinctive renal vascular injury. The hallmark lesion is concentric intimal proliferation (onion-skin lesion) of the interlobular and arcuate arteries, leading to luminal occlusion and reduced renal perfusion. This triggers activation of the renin–angiotensin–aldosterone system (RAAS), producing severe hypertension and further renal ischaemia, creating a vicious cycle.
Key pathological and mechanistic features include:
- Intimal proliferation: Fibroblast and myofibroblast proliferation within arteriolar intima, producing a concentric "onion-skin" appearance on renal biopsy.
- Microangiopathic haemolytic anaemia (MAHA): Red cell fragmentation through narrowed arterioles produces schistocytes, elevated LDH, and low haptoglobin.
- RAAS activation: Renal ischaemia drives renin release, causing severe hypertension — often with disproportionately elevated diastolic pressures.
- Endothelial dysfunction: Endothelin-1 upregulation and reduced nitric oxide contribute to vasospasm and vascular remodelling.
- Thrombotic microangiopathy: In a subset, complement dysregulation may contribute to a TMA phenotype.
Risk Factors for SRC
| Risk Factor | Association | Notes |
|---|---|---|
| Diffuse cutaneous SSc | Strong (highest risk subset) | ~80% of SRC cases are dcSSc; risk highest in first 3–5 years |
| Anti-RNA polymerase III antibodies | Very strong | OR ~5–8; present in 40–60% of SRC patients |
| Corticosteroids ≥15 mg/day | Strong | Dose-dependent risk; use lowest possible dose in early dcSSc |
| New anaemia | Moderate | May indicate MAHA or renal failure |
| Large joint contractures | Moderate | Reflects extensive skin/tendon involvement |
| Rapid skin score progression | Moderate | Rising modified Rodnan skin score (mRSS) correlates with SRC risk |
| Myopathy / elevated CK | Moderate | Concurrent skeletal muscle involvement |
| Anti-centromere antibodies | Protective | Strongly associated with limited cutaneous SSc; SRC rare in ACA+ patients |
| Calcium channel blockers | Possible trigger | Theoretical risk of reducing renal perfusion; generally advised caution in early dcSSc |
Clinical Features & Presentation
SRC typically presents acutely in a patient with known SSc, although it may occasionally be the first manifestation of previously undiagnosed systemic sclerosis (particularly in older males). The classic presentation is:
Key Clinical Features
- Hypertension: New or significantly accelerated; often diastolic predominant. Note: ~10% of SRC cases present as "normotensive SRC" — particularly in patients with pre-existing low baseline BP or concurrent scleroderma cardiac involvement.
- AKI: Rapidly rising creatinine (often doubling within days to weeks); oliguria or anuria in severe cases.
- MAHA: Microangiopathic haemolytic anaemia with schistocytes on blood film, elevated LDH, undetectable haptoglobin, and thrombocytopaenia.
- Hypertensive retinopathy: Fundoscopy may reveal cotton-wool spots, flame haemorrhages, papilloedema.
- Pulmonary oedema: May be cardiogenic (hypertensive) or non-cardiogenic (capillary leak); can develop rapidly.
- Encephalopathy: Headache, confusion, seizures, visual disturbance in severe cases.
- Microscopic haematuria and proteinuria: Usually mild; nephrotic-range proteinuria is uncommon and suggests an alternative or concurrent diagnosis.
Investigations & Diagnosis
SRC is primarily a clinical diagnosis based on new-onset hypertension and AKI in a patient with SSc. Investigations support the diagnosis and exclude mimics. Do not delay ACE inhibitor therapy while awaiting results.
Essential Investigations
Diagnostic Criteria
There is no single pathognomonic test. SRC is diagnosed when a patient with SSc (typically early dcSSc) develops:
- New or accelerated hypertension (usually BP >150/90 mmHg, or >30/20 mmHg above baseline)
- AKI (creatinine rise >50% from baseline or >1.5× baseline)
- ± features of MAHA (schistocytes, ↑LDH, ↓haptoglobin, ↓platelets)
- ± elevated plasma renin
Management
SRC management centres on aggressive RAAS blockade with ACE inhibitors, supportive care, dialysis if required, and multidisciplinary involvement (rheumatology, nephrology, ICU). Treatment should never be delayed.
First-Line: ACE Inhibitors
ACE inhibitors are the cornerstone of SRC treatment and the single most important intervention. They block the pathological RAAS activation driving SRC. Initiate immediately at the first clinical suspicion.
Blood Pressure Targets & Monitoring
Second-Line & Adjunctive Agents
If BP is not adequately controlled with maximal ACE inhibitor doses, add:
Agents to Avoid
- Calcium channel blockers (non-dihydropyridine): Verapamil and diltiazem may impair renal perfusion and worsen Raynaud's. Dihydropyridines (amlodipine) are acceptable as add-on therapy.
- Beta-blockers: Generally avoided in SSc due to worsening of Raynaud's phenomenon; use only if compelling cardiac indication.
- NSAIDs: Contraindicated — nephrotoxic, worsen renal perfusion, may precipitate SRC.
- High-dose corticosteroids: ≥15 mg/day prednisolone equivalent is an independent risk factor for SRC.
Dialysis
Approximately 50–70% of SRC patients will require dialysis at some point during the acute illness. Indications for dialysis are the same as for other causes of AKI:
- Refractory hyperkalaemia despite medical management
- Severe metabolic acidosis (pH <7.1)
- Fluid overload with pulmonary oedema unresponsive to diuretics
- Uraemic symptoms (encephalopathy, pericarditis)
- Oligoanuria (<200 mL/24h) with progressive uraemia
Key principle: Continue ACE inhibitors even when dialysis is commenced. Renal recovery may occur weeks to months after SRC onset, particularly with ongoing RAAS blockade. Studies show that 40–55% of patients initially requiring dialysis eventually become dialysis-independent, especially if ACE inhibitor therapy is maintained.
Emerging & Adjunctive Therapies
- Bosentan (endothelin receptor antagonist): Case reports and small series suggest potential benefit in refractory SRC. Not PBS-listed for this indication; requires specialist initiation and authority application.
- Eculizumab (complement C5 inhibitor): Considered if a complement-mediated TMA phenotype is suspected. Highly expensive; requires Haematology/Renal specialist input.
- Plasma exchange: May be considered if TTP cannot be excluded (while awaiting ADAMTS13 results) or in severe TMA without response to ACE inhibitors. Generally limited role in SRC itself.
- Prostacyclin analogues (iloprost IV): May improve renal perfusion and digital ulceration; specialist use only.
Supportive Care
- Fluid and electrolyte management — monitor K⁺ closely (RAAS blockade + AKI → hyperkalaemia risk)
- ECG monitoring for arrhythmias in severe cases
- Manage pulmonary oedema (diuretics, NIV, or dialysis as indicated)
- Nutritional support — consider dietitian input
- Psychological support — SSc with SRC carries high morbidity and mortality; patients and families require ongoing counselling
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander Australians experience a higher burden of autoimmune rheumatic diseases and chronic kidney disease compared to non-Indigenous Australians. While specific data on SRC in ATSI populations are limited, several factors contribute to disparities in outcomes:
📚 References
- 1. Woodworth TG, Suliman YA, Li W, Furst DE, Clements P. Scleroderma renal crisis and renal outcomes in systemic sclerosis patients: a systematic review and meta-analysis. Rheumatology (Oxford). 2023;62(3):1023–1034.
- 2. Guillevin L, Bérezné A, Seror R, et al. Scleroderma renal crisis: a retrospective multicentre study on 91 patients and 427 controls. Rheumatology (Oxford). 2012;51(3):460–467.
- 3. Penn H, Howie AJ, Kingdon EJ, et al. Scleroderma renal crisis: patient characteristics and long-term outcomes. QJM. 2007;100(8):485–494.
- 4. Steen VD, Medsger TA Jr. Case-control study of corticosteroids and other drugs that either precipitate or protect from the development of scleroderma renal crisis. Arthritis Rheum. 1998;41(9):1613–1619.
- 5. Hissaria P, Lester S, Hakendorf P, et al. Survival in scleroderma: results from the population-based South Australian Register. Intern Med J. 2011;41(5):381–390.
- 6. Dobrota R, Mihai C, Distler O. Renal involvement in systemic sclerosis: an update on scleroderma renal crisis. Rheumatology (Oxford). 2022;61(3):934–944.
- 7. Mecoli CA, Shah AA, Boin F, Wigley FM. The management of scleroderma renal crisis. Curr Opin Rheumatol. 2021;33(6):514–520.
- 8. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease in Aboriginal and Torres Strait Islander people. Cat. no. PHE 261. Canberra: AIHW; 2023.
- 9. Nikpour M, Hissaria P, Byron J, et al. Prevalence, correlates and clinical usefulness of antibodies to RNA polymerase III in systemic sclerosis: a cross-sectional analysis of data from an Australian cohort. Arthritis Res Ther. 2011;13(6):R211.
- 10. Teixeira L, Mouthon L, Mahr A, et al. Mortality and risk factors of scleroderma renal crisis: a French retrospective study of 50 patients. Ann Rheum Dis. 2008;67(1):110–116.
- 11. Kowal-Bielecka O, Fransen J, Avouac J, et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Ann Rheum Dis. 2017;76(8):1327–1339.
- 12. Hudson M, Baron M, Tatibouet S, Furst DE, Khanna D. Exposure to ACE inhibitors prior to the onset of scleroderma renal crisis — results from the International Scleroderma Renal Crisis Survey. Semin Arthritis Rheum. 2018;48(3):466–470.