📋 Key Information Summary
- IgA nephropathy (Berger's disease) is the most common primary glomerulonephritis worldwide and the leading cause of GN-related end-stage kidney disease (ESKD) in young adults aged 20–40 years in Australia.
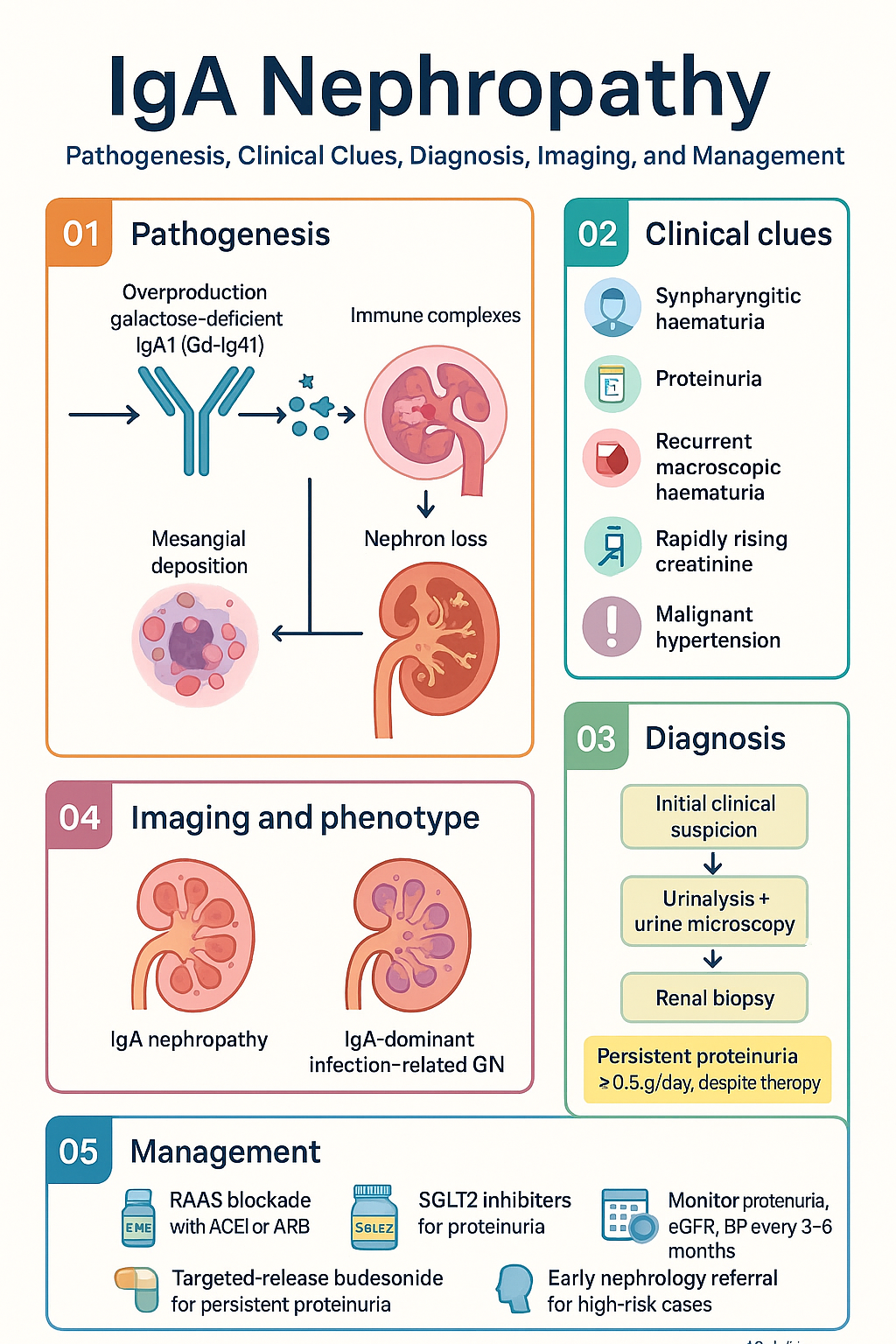
- Pathogenesis centres on galactose-deficient IgA1 (Gd-IgA1): aberrantly glycosylated IgA1 forms immune complexes that deposit in the mesangium, triggering complement activation and progressive nephron loss.
- Classic presentation: synpharyngitic haematuria — visible (macroscopic) haematuria within 1–2 days of an upper respiratory tract infection, with or without proteinuria.
- Diagnosis requires renal biopsy: mesangial IgA (± C3) deposits on immunofluorescence with mesangial hypercellularity on light microscopy (Oxford/MEST-C classification).
- Risk stratify using the International IgA Nephropathy Prediction Tool (IIgAN-PT) to guide intensity of therapy.
- First-line therapy for all patients: maximum-tolerated RAAS blockade — ACE inhibitor (ACEi) or ARB titrated to reduce proteinuria <0.5–1 g/day and systolic BP <125 mmHg.
- SGLT2 inhibitors (dapagliflozin or empagliflozin) are now recommended as add-on therapy for proteinuria ≥0.5 g/day with eGFR ≥20 mL/min/1.73 m², independent of diabetes status.
- Targeted-release budesonide (Nefecon® / TARPEYO®) is PBS-listed (Authority Required) for IgAN with persistent proteinuria ≥1 g/day despite optimised RAAS blockade, reducing Gd-IgA1 via gut mucosal immunomodulation.
- Immunosuppression (cyclophosphamide, mycophenolate, corticosteroids) is reserved for rapidly progressive or high-risk disease; do NOT use as first-line in all patients.
- Tonkin et al. STOP-IgA and TESTING trials demonstrated systemic corticosteroids reduce proteinuria but carry significant infection risk — use with caution.
- ATSI populations have higher rates of ESKD and often present later; culturally safe engagement and early nephrology referral are essential.
- Monitor proteinuria (uACR), eGFR, BP, and pregnancy status every 3–6 months; refer to nephrology if eGFR declining >5 mL/min/year or proteinuria >1 g/day despite therapy.
- Novel targeted therapies including iptacopan (complement factor B inhibitor) and narsoplimab (MASP-2 inhibitor) are in late-phase trials and may alter the treatment paradigm.
Introduction & Australian Epidemiology
IgA nephropathy (IgAN), also known as Berger's disease, is the most common primary glomerulonephritis (GN) worldwide and a leading cause of kidney failure in young adults. It is characterised by the deposition of galactose-deficient IgA1 (Gd-IgA1) immune complexes in the glomerular mesangium, triggering mesangial proliferation, complement activation, and progressive nephron loss.
In Australia, IgAN accounts for approximately 10–20% of all primary GN diagnoses on renal biopsy, with the highest incidence in individuals aged 20–40 years. There is a 2:1 male predominance. Aboriginal and Torres Strait Islander peoples experience disproportionately higher rates of glomerular disease overall, though IgAN remains less common than in non-Indigenous populations — lupus nephritis and glomerulosclerosis are more prevalent in ATSI communities.
Disease course is highly variable: up to 40% of patients will progress to ESKD within 20 years of diagnosis if untreated. Early identification, risk stratification, and timely initiation of renin–angiotensin system (RAS) blockade are the cornerstones of management. Recent advances — including SGLT2 inhibitors and targeted-release budesonide — have expanded the therapeutic armamentarium and shifted the paradigm away from empirical immunosuppression.
This guideline synthesises current evidence from the TESTING trial, STOP-IgA, NefIgArd, and KDIGO 2024 update, contextualised for Australian practice including PBS availability, MBS billing, and ATSI health considerations.
Pathogenesis — Galactose-Deficient IgA1
The pathogenesis of IgAN is best understood as a multi-hit process:
- Hit 1 — Overproduction of Gd-IgA1: Peyer's patches and mucosa-associated lymphoid tissue (MALT) in the gut produce abnormally glycosylated IgA1 with deficient galactose residues on the hinge-region O-linked glycans. This is driven by mucosal immune dysregulation, often triggered by respiratory or gastrointestinal infections.
- Hit 2 — Anti-glycan antibody production: The host mounts IgG or IgA autoantibodies against the exposed N-acetylgalactosamine (GalNAc) epitopes on Gd-IgA1, forming circulating immune complexes (CICs).
- Hit 3 — Mesangial deposition: CICs deposit in the glomerular mesangium via interactions with fibronectin and integrin receptors, activating mesangial cell proliferation and extracellular matrix expansion.
- Hit 4 — Complement activation and injury: Mesangial deposits activate the lectin pathway (via MBL/MASP-2), alternative pathway (via factor B), and classical pathway, generating C5a and the membrane attack complex (MAC), driving tubulointerstitial fibrosis and progressive nephron loss.
Key Pathological Findings (Oxford MEST-C Classification)
| Score | Parameter | Definition | Prognostic Significance |
|---|---|---|---|
| M0/M1 | Mesangial hypercellularity | <4 vs ≥4 mesangial cells per mesangial area | M1 predicts faster progression |
| E0/E1 | Endocapillary hypercellularity | Absent vs present | E1 associated with active inflammation; may respond to immunosuppression |
| S0/S1 | Segmental sclerosis | Absent vs present | S1 predicts worse renal outcome |
| T0/T1/T2 | Tubular atrophy / interstitial fibrosis | <25% / 25–50% / >50% | T1 and T2 are the strongest histological predictors of ESKD |
| C0/C1/C2 | Crescents (cellular/fibrocellular) | None / <50% / ≥50% of glomeruli | C2 indicates aggressive disease; consider immunosuppression |
Clinical Features & Diagnostic Criteria
Classic Presentation: Synpharyngitic Haematuria
The hallmark presentation of IgAN is synpharyngitic (or "synpharyngitic") haematuria — visible haematuria appearing within 24–48 hours of an upper respiratory tract infection (URTI), pharyngitis, or less commonly, gastroenteritis. This rapid onset distinguishes it from post-streptococcal GN, where haematuria appears 1–3 weeks after infection.
Episodes typically last 2–5 days and may be accompanied by:
- Dark brown or "cola-coloured" urine
- Mild loin or flank pain (bilateral)
- Low-grade fever during the precipitating infection
- Transient oedema (rare unless nephrotic-range proteinuria)
Other Presentations
| Presentation | Frequency | Features |
|---|---|---|
| Synpharyngitic haematuria | 40–50% (children up to 80%) | Macroscopic haematuria 1–2 days post-URTI |
| Asymptomatic haematuria / proteinuria | 30–40% | Incidental finding on urinalysis or health screen |
| Nephrotic syndrome | 5% | Oedema, heavy proteinuria >3.5 g/day; consider concurrent minimal change disease |
| Rapidly progressive GN (RPGN) | <5% | Rapid rise in creatinine over weeks, crescentic histology (MEST-C C2); urgent nephrology |
| Malignant hypertension | <5% | BP >180/120, papilloedema, AKI; emergency management required |
When to Suspect IgAN
- Recurrent macroscopic haematuria associated with URTI in a young adult (20–40 years)
- Persistent microscopic haematuria with dysmorphic red cells or red cell casts on urine microscopy
- Isolated proteinuria 0.2–3.5 g/day with normal renal function in a young patient
- Haematuria with concurrent low C3 (suggesting complement activation) but normal C4
Investigations & Renal Biopsy
Baseline Investigations
Renal Biopsy — Gold Standard
Definitive diagnosis of IgAN requires a percutaneous renal biopsy with immunofluorescence (IF) and electron microscopy (EM).
Histopathological Criteria for IgAN Diagnosis
| Modality | Finding | Comment |
|---|---|---|
| Light microscopy | Mesangial hypercellularity, matrix expansion | May show focal/diffuse proliferative pattern; classify by MEST-C |
| Immunofluorescence (IF) | IgA dominant mesangial deposits (≥2+ on 0–3 scale) | Diagnostic criterion; C3 co-deposits in >90%; IgG or IgM may co-deposit |
| Electron microscopy (EM) | Electron-dense mesangial deposits | Confirms IF findings; subendothelial or subepithelial deposits suggest other diagnoses (e.g., lupus nephritis, IgA-dominant infection-related GN) |
Risk Stratification & Prognosis
The International IgA Nephropathy Prediction Tool (IIgAN-PT), developed by the IgA Nephropathy Network (NEPTUNE/CureGN), is the preferred validated risk calculator. It integrates clinical and histological variables at the time of biopsy to estimate 5-year and 7-year risk of a 50% decline in eGFR or ESKD.
Clinical Risk Factors for Progression
- Persistent proteinuria >1 g/day despite RAAS blockade
- Hypertension (BP >140/90 or requiring antihypertensives)
- Reduced eGFR (<60 mL/min/1.73 m²) at presentation
- Histological MEST-C scores: M1, E1, S1, T1/T2, C1/C2
- Older age at diagnosis
- Male sex
- Obesity (BMI >30 kg/m²) and metabolic syndrome
Management
Management of IgAN is stratified by proteinuria level, eGFR, and histological risk. The current therapeutic approach follows a layered strategy: supportive care first, then targeted therapies for higher-risk disease.
Layer 1 — Supportive / Foundation Therapy (All Patients)
RAAS Blockade — ACE Inhibitors or ARBs
Maximum-tolerated RAAS blockade is the cornerstone of IgAN management. ACEi or ARB should be titrated to achieve:
- Proteinuria <0.5–1 g/day (target <0.5 g/day ideal)
- Systolic BP <125 mmHg (or <130 mmHg if tolerated poorly)
- Avoid combining ACEi + ARB (ONTARGET trial — no benefit, increased harm)
Layer 2 — SGLT2 Inhibitors
Based on the DAPA-CKD and EMPA-KIDNEY trials, SGLT2 inhibitors reduce proteinuria and slow eGFR decline in CKD including IgAN. They are recommended as add-on therapy for all IgAN patients with:
- Proteinuria ≥0.5 g/day
- eGFR ≥20 mL/min/1.73 m²
- On maximised RAAS blockade
- Independent of diabetes status
Layer 3 — Targeted-Release Budesonide (Nefecon®)
NefIgArd trial evidence: The phase 3 NefIgArd trial demonstrated that Nefecon® 16 mg/day for 9 months (followed by 3 months washout) significantly reduced proteinuria (26% relative reduction vs placebo) and stabilised eGFR compared with supportive care alone. The benefit was sustained at 2-year follow-up.
Layer 4 — Immunosuppression (Specialist-Only)
Systemic immunosuppression is reserved for high-risk or rapidly progressive disease. It should be initiated only by a nephrologist after optimising supportive therapy (Layers 1–3).
Systemic Corticosteroids
The TESTING trial (2022 update) showed that a modified-dose methylprednisolone/prednisolone regimen reduced the risk of 40% eGFR decline or ESKD by 47%, but was associated with serious infections. The reduced-dose regimen (0.4 mg/kg/day prednisolone, max 32 mg/day, tapered over 6–8 months) has a more favourable safety profile.
Other Immunosuppressive Options (Specialist Use)
| Agent | Indication | Dose | PBS Status |
|---|---|---|---|
| Mycophenolate mofetil (CellCept®) | Consider in Asian populations with M1E1 disease (variable evidence); not first-line in Caucasians | 1 g PO BD for 12–24 months | PBS General Benefit (for transplant, not IgAN PBS-listed indication) |
| Cyclophosphamide | Crescentic/RPGN IgAN (MEST-C C2); rapidly progressive disease | 2 mg/kg/day PO for 2–3 months (or IV pulse 500–750 mg/m² monthly × 6) | PBS General Benefit |
| Azathioprine | Maintenance after cyclophosphamide (if steroid-sparing needed) | 2 mg/kg/day PO; check TPMT prior | PBS General Benefit |
| Rituximab | Case series data only; NOT recommended routinely for IgAN | 1000 mg IV × 2 doses (day 1 and day 15) | class="guideline-td">PBS Authority Required (for specific indications only)
Novel & Emerging Therapies (2024–2025)
The therapeutic landscape for IgAN is evolving rapidly. The following agents are in advanced clinical trials and may change practice in the near future:
- Iptacopan (complement factor B inhibitor): APPLAUSE-IgAN phase 3 trial demonstrated significant proteinuria reduction. May target the alternative complement pathway implicated in IgAN progression.
- Narsoplimab (anti-MASP-2 monoclonal antibody): Blocks lectin pathway activation. Phase 2/3 data in IgAN; TGA not yet approved.
- Sibeprenlimab (anti-APRIL antibody): Reduces IgA and Gd-IgA1 production. Phase 2 trial (ENVISION) showed significant proteinuria reduction.
- Atacicept (TACI-Ig fusion protein): Inhibits BAFF and APRIL, reducing IgA-producing B cells. Phase 2 results promising.
- Zigakibart (anti-APRIL antibody): Another APRIL-targeting agent with phase 3 trial underway.
These agents are not yet PBS-listed or TGA-approved for IgAN as of 2025. Refer to clinicaltrials.gov for trial enrolment eligibility.
Monitoring & Follow-Up
Monitoring Schedule
When to Refer to Nephrology
- All newly diagnosed IgAN patients — initial nephrology assessment recommended
- Proteinuria >0.5 g/day despite 3–6 months of optimised RAAS blockade
- eGFR declining >5 mL/min/year
- eGFR <30 mL/min/1.73 m² (pre-dialysis planning)
- Nephrotic syndrome or rapidly progressive GN
- Pregnancy planning (ACEi/ARB cessation required)
- Consideration for immunosuppression or clinical trial enrolment
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of kidney disease in Australia. While IgA nephropathy is less common in ATSI populations than non-Indigenous Australians, the overall rate of ESKD is 8–10 times higher in Indigenous communities (AIHW 2023). Glomerulonephritis in ATSI peoples is more often due to lupus nephritis, post-infectious GN, and glomerulosclerosis associated with obesity and diabetes.
When IgAN does occur in ATSI patients, late presentation, reduced access to specialist nephrology services, and comorbid conditions (diabetes, cardiovascular disease, obesity) may worsen outcomes. The following considerations are essential:
Quick Reference — Treatment Summary
📚 References
- 1. KDIGO 2024 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney International. 2024;105(4S):S1–S276. doi:10.1016/j.kint.2023.10.016
- 2. Barratt J, Lafayette RA, Rovin BH, et al. NefIgArd: Phase 3 Trial of Nefecon in IgA Nephropathy. Nature Medicine. 2023;29:1024–1033. doi:10.1038/s41591-023-02275-z
- 3. Barratt J, Rovin BH, Rauseo V, et al. The evolving treatment landscape of IgA nephropathy. Nature Reviews Nephrology. 2024;20(2):87–103. doi:10.1038/s41581-023-00780-7
- 4. Wheeler DC, Toto RD, Stefansson BV, et al. A pre-specified analysis of the DAPA-CKD trial: effect of dapagliflozin on kidney outcomes in patients with IgA nephropathy. Kidney International. 2021;99(4):874–884. doi:10.1016/j.kint.2020.12.010
- 5. The EMPA-KIDNEY Collaborative Group. Empagliflozin in Patients with Chronic Kidney Disease. New England Journal of Medicine. 2023;388(2):117–127. doi:10.1056/NEJMoa2204233
- 6. Lv J, Zhang H, Wong MG, et al. Effect of oral methylprednisolone on clinical outcomes in patients with IgA nephropathy: The TESTING randomized clinical trial. JAMA. 2017;318(5):432–442. doi:10.1001/jama.2017.9362
- 7. Rauen T, Eitner F, Fitzner C, et al. Intensive supportive care plus immunosuppression in IgA nephropathy (STOP-IgA). New England Journal of Medicine. 2015;373(23):2225–2236. doi:10.1056/NEJMoa1419128
- 8. Trimarchi H, Barratt J, Cattran DC, et al. Oxford Classification of IgA nephropathy 2016: an update from the IgA Nephropathy Classification Working Group. Kidney International. 2017;91(5):1014–1021. doi:10.1016/j.kint.2017.02.003
- 9. Barbour SJ, Coppo R, Zhang H, et al. Evaluating a new International Risk-Prediction Tool in IgA Nephropathy. JAMA Internal Medicine. 2019;179(6):743–750. doi:10.1001/jamainternmed.2019.0603
- 10. Australian Institute of Health and Welfare (AIHW). Chronic kidney disease: Australian facts. Cat. no. PHE 229. Canberra: AIHW; 2023.
- 11. RHDAustralia (a program of NACCHO). Recommendations for the diagnosis and management of chronic kidney disease in Aboriginal and Torres Strait Islander peoples. Darwin: RHDAustralia; 2023.
- 12. Kidney Health Australia. Chronic Kidney Disease (CKD) Management in Primary Care. 5th ed. Melbourne: Kidney Health Australia; 2024.
- 13. Rizk DV, Saha MK, Hall S, et al. Complement as a target in IgA nephropathy. Kidney International. 2023;104(5):893–907. doi:10.1016/j.kint.2023.06.028
- 14. Pharmaceutical Benefits Scheme (PBS). Nefecon (Nefecon) capsules. PBS Schedule. Australian Government Department of Health and Aged Care. Available at: pbs.gov.au. Accessed 2025.