📋 Key Information Summary
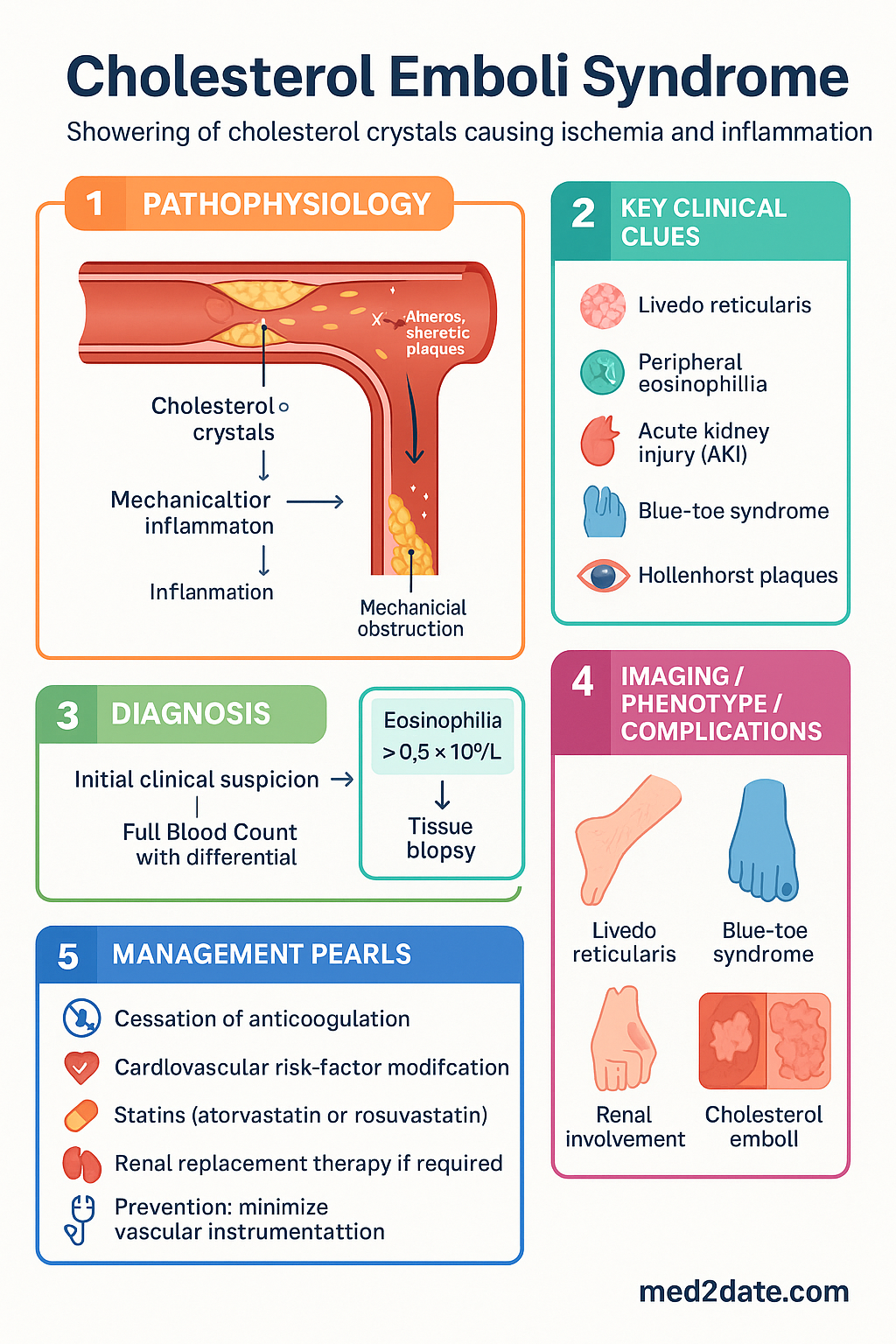
- Cholesterol emboli syndrome (CES) results from showering of cholesterol crystals from eroded atherosclerotic plaques into small-to-medium arteries, causing downstream ischaemia and an intense inflammatory response.
- Classic triggers: vascular catheterisation, arterial surgery, thrombolysis, and anticoagulation (especially heparin or warfarin initiation/escalation) in patients with severe aortic or iliac atherosclerosis.
- Triad of presentation: livedo reticularis, peripheral eosinophilia, and acute kidney injury (AKI) — though the complete triad is present in fewer than one-third of cases.
- AKI onset: typically delayed 1–8 weeks post-procedure (mean 2–4 weeks), distinguishing CES from contrast-associated AKI which peaks at 48–72 hours.
- Blue-toe syndrome: painful, cyanotic toes with palpable pedal pulses is a hallmark finding of cholesterol microembolisation to the lower limbs.
- Eosinophilia occurs in 60–80 % of cases; hypereosinophilia (>1.5 × 10⁹/L) is a red flag. Eosinophiluria may also be present.
- Hollenhorst plaques on fundoscopy — bright, refractile emboli at arterial bifurcations — are a specific clue when present.
- Diagnosis is primarily clinical in the context of a suggestive trigger; tissue biopsy (skin, kidney) showing biconvex, needle-shaped clefts in arterioles is confirmatory but often unnecessary.
- There is no proven pharmacotherapy to dissolve or clear cholesterol emboli. Management is supportive: cessation of anticoagulation where feasible, aggressive cardiovascular risk-factor modification (statins, antihypertensives, antiplatelet therapy), and renal replacement therapy if required.
- Statins (atorvastatin or rosuvastatin) are strongly recommended — observational data suggest improved survival and renal outcomes through plaque stabilisation and anti-inflammatory effects.
- Mortality is high: in-hospital mortality 16–26 %; 1-year mortality approaches 40–60 % in hospitalised cohorts, driven largely by cardiovascular events and progression to end-stage kidney disease.
- Prevention is paramount — minimise vascular instrumentation, use radial or distal access where possible, and consider atheroembolic risk in patients with known aortic plaques ≥4 mm or mobile atheroma on echocardiography.
- Renal prognosis: approximately 25–30 % of patients require long-term dialysis; partial recovery may occur over months if further embolisation is prevented.
Introduction & Australian Epidemiology
Cholesterol emboli syndrome (CES) — also termed atheroembolic renal disease or cholesterol crystal embolisation — results from the showering of atherosclerotic plaque material into renal and other end-organ vessels, most commonly following vascular procedures, arterial surgery, thrombolysis, or anticoagulation therapy.
The disorder was first described by Flory in 1945 at autopsy in patients with severe aortic atherosclerosis. With the proliferation of endovascular procedures, cardiac catheterisation, and percutaneous coronary intervention (PCI), clinically apparent CES has become an increasingly recognised cause of acute kidney injury (AKI) and multisystem organ dysfunction.
Australian Context
Australia's ageing population and high burden of cardiovascular disease place many older Australians at risk. Approximately 180,000 coronary angiography procedures are performed annually in Australia, and a further 25,000–30,000 peripheral vascular interventions add to the population at risk. The true incidence of clinically apparent CES is estimated at 0.5–2 % of patients undergoing catheter-based vascular procedures, though subclinical embolisation (detected on renal biopsy) may occur in up to 25–30 % of post-mortem studies in patients with severe aortic atherosclerosis.
CES disproportionately affects men (male:female ratio approximately 3–4:1), typically presenting in the 6th–8th decade of life. Patients with known abdominal aortic aneurysm, diffuse iliofemoral disease, prior aortic valve replacement, or mobile aortic arch atheroma on transoesophageal echocardiography (TOE) are at highest risk.
Data from the Australian Institute of Health and Welfare (AIHW) and the ANZDATA Registry indicate that atheroembolic disease accounts for a small but significant proportion of hospital-acquired AKI, particularly in tertiary centres performing high volumes of endovascular work. Importantly, CES is thought to be substantially underdiagnosed, as the clinical features overlap with contrast-associated AKI, vasculitis, and nephrosclerosis.
Pathophysiology & Triggers
Mechanism of Embolisation
Cholesterol emboli arise from the rupture or erosion of atherosclerotic plaques, most commonly in the abdominal aorta, iliac arteries, or aortic arch. When the fibrous cap of a plaque is disrupted — by mechanical trauma (catheter passage, cross-clamping), thrombolytic dissolution of protective thrombus, or changes in haemodynamic shear stress — cholesterol crystals, necrotic lipid debris, and platelet-fibrin aggregates are released into the arterial circulation.
These emboli are typically 100–200 µm in diameter and lodge in small arterioles of the kidneys, skin, gastrointestinal tract, retina, brain, and skeletal muscle. Unlike thromboemboli, cholesterol crystals are rigid and cannot be lysed by fibrinolytic agents. Once impacted, they provoke a biphasic vascular response:
- Acute phase (hours–days): mechanical obstruction of arteriolar lumen, platelet adhesion, and endothelial damage.
- Subacute phase (days–weeks): intense intimal proliferation, giant-cell foreign-body reaction around the biconvex needle-shaped cholesterol clefts, and fibrosis — leading to progressive arteriolar occlusion and organ ischaemia.
This delayed inflammatory response explains the characteristic latency of 1–8 weeks between the embolic event and peak clinical manifestations, particularly progressive renal impairment.
Precipitating Triggers
| Trigger Category | Specific Triggers | Relative Risk |
|---|---|---|
| Endovascular procedures | Coronary angiography, peripheral angioplasty, aortic stenting, endovascular aneurysm repair (EVAR), intra-aortic balloon pump insertion | High — most common identifiable cause |
| Vascular surgery | Aortic cross-clamping, aortic valve replacement, aortobifemoral bypass, carotid endarterectomy | High — 1–3 % post-aortic surgery |
| Anticoagulation | Heparin (UFH or LMWH) initiation, warfarin initiation or dose escalation, DOACs (less commonly reported) | Moderate — may dissolve protective mural thrombus |
| Thrombolytic therapy | IV alteplase for STEMI, catheter-directed thrombolysis for PE or limb ischaemia | Moderate |
| Spontaneous | No identifiable iatrogenic trigger — may occur with plaque progression, severe hypertension, or haemodynamic stress | Low (but increasingly recognised) |
Anatomical Risk Factors
The following anatomical features significantly increase the risk of CES:
- Aortic plaque thickness ≥ 4 mm (OR 3.2) or mobile atheroma on TOE
- Abdominal aortic aneurysm with intraluminal thrombus
- Diffuse aortoiliac occlusive disease
- Porcelain aorta (heavily calcified ascending aorta)
- Previous prosthetic aortic valve — atheromatous degeneration at the annular site
Clinical Features (Livedo, Eosinophilia, AKI)
CES is a multisystem disorder. Cholesterol crystals embolise to virtually any organ, producing a protean clinical picture. The onset is typically delayed 1–14 days after the embolic insult, with progressive worsening over 2–8 weeks as the inflammatory response evolves.
Classic Triad
The textbook triad — present simultaneously in approximately 25–30 % of patients — comprises:
- Livedo reticularis — a violaceous, net-like mottling of the skin, typically affecting the lower limbs, buttocks, and trunk. Results from arteriolar occlusion in the dermal and subdermal vascular plexus. May progress to skin necrosis or gangrene.
- Eosinophilia — peripheral eosinophil count >0.5 × 10⁹/L, present in 60–80 % of cases. Hypereosinophilia (>1.5 × 10⁹/L) occurs in 15–25 %. May be transient and missed if the full blood count is not monitored serially. Eosinophiluria (Wright stain or Hansel stain of urine sediment) may also be detected.
- Acute kidney injury (AKI) — typically non-oliguric, progressive over days to weeks, with bland urinary sediment (few casts, minimal proteinuria). Bilateral renal embolisation is the rule. Creatinine may rise gradually over weeks before plateauing.
Peripheral Vascular Manifestations
- Blue-toe syndrome: sudden onset of painful, cyanotic, often gangrenous toes with preserved pedal pulses — the hallmark of digital embolisation. Present in 35–50 % of CES patients.
- Livedo reticularis / racemosa: as above; may be associated with tender subcutaneous nodules.
- Peripheral gangrene: in severe cases; may necessitate amputation.
- Myalgia: diffuse limb pain from skeletal muscle ischaemia.
Renal Manifestations
- AKI: the most common presentation prompting investigation. Typically non-oliguric; urine microscopy shows bland sediment, mild proteinuria (<1 g/day), and occasional eosinophiluria.
- Hypertension: new or worsened hypertension due to renin-mediated responses from ischaemic nephrons (renovascular-type mechanism).
- Haematuria: may be present but is typically mild; gross haematuria is uncommon.
- Flank pain: occasionally reported due to renal infarction.
Systemic & Extrarenal Features
| Organ System | Features | Frequency |
|---|---|---|
| Ocular | Hollenhorst plaques (refractile emboli at retinal arteriolar bifurcations); visual field defects; amaurosis fugax | 10–25 % |
| Gastrointestinal | Abdominal pain, GI bleeding, nausea/vomiting, pancreatitis, bowel infarction | 15–30 % |
| Neurological | Transient ischaemic attack (TIA), stroke, confusion, spinal cord ischaemia | 10–20 % |
| Cardiac | Myocardial infarction (Type 2), pericarditis, new heart failure | 5–10 % |
| Constitutional | Fever, weight loss, malaise, myalgia, anorexia | 40–60 % |
Temporal Patterns
Investigations & Diagnosis
Diagnosis of CES is primarily clinical, based on the temporal association with a known trigger, compatible clinical features (livedo, eosinophilia, AKI, blue-toe syndrome), and exclusion of alternative diagnoses. There is no single pathognomonic test, though tissue biopsy provides definitive confirmation.
Laboratory Investigations
Imaging
Tissue Biopsy
Biopsy of affected tissue is the gold standard for diagnosis. Findings on histology:
- Pathognomonic finding: biconvex, needle-shaped cholesterol clefts within arteriolar lumina (visible on H&E as empty, slit-like spaces — cholesterol is dissolved during processing).
- Associated features: intimal proliferation, giant-cell foreign-body reaction, fibrin thrombi, and arteriolar fibrosis.
- Skin biopsy: most accessible site — punch biopsy of livedo lesions or blue toes carries high diagnostic yield (~75 %) and low morbidity.
- Renal biopsy: higher diagnostic yield but greater procedural risk in anticoagulated or azotaemic patients. Reserve for diagnostic uncertainty when skin biopsy is non-diagnostic.
- MBS item: Skin biopsy (MBS item 30071/30072); renal biopsy by nephrologist (discuss with renal unit — MBS item applies).
Diagnostic Criteria
No universally accepted diagnostic criteria exist, but the following framework is widely used:
Management & Prognosis
Immediate Management
1. Cessation or Avoidance of Trigger
- Anticoagulation: if CES is triggered by anticoagulation initiation/escalation, discontinue if clinically safe. This is the single most important intervention. The decision must balance thrombotic risk (e.g., mechanical heart valve, recent DVT/PE) against the risk of ongoing embolisation.
- Avoid further vascular instrumentation: postpone elective catheterisation and surgery.
- Thrombolysis: discontinue if suspected.
2. Supportive Care
- Fluid and electrolyte management; avoid nephrotoxins (NSAIDs, iodinated contrast, aminoglycosides).
- Renal replacement therapy (haemodialysis or peritoneal dialysis) if indicated by standard criteria (refractory hyperkalaemia, acidosis, volume overload, uraemic symptoms).
- Wound care for skin lesions and gangrenous toes; podiatric and vascular surgery input as needed.
- Adequate analgesia for limb ischaemia and skin ulceration.
Pharmacological Management
No randomised controlled trials have demonstrated efficacy for any specific therapy in CES. The following are recommended based on observational data, pathophysiological rationale, and expert consensus:
Therapies NOT Recommended
| Therapy | Rationale Against Use |
|---|---|
| Anticoagulation (heparin, warfarin) | May worsen embolisation by dissolving protective mural thrombus; no evidence of benefit. Avoid unless compelling thrombotic indication (e.g., mechanical heart valve). |
| Thrombolysis (alteplase, tenecteplase) | Cannot dissolve cholesterol crystals. Carries bleeding risk. No role in CES. |
| Corticosteroids | Often empirically given for eosinophilia. No proven benefit in CES; eosinophilia typically self-resolves. May mask concurrent infection. |
| Prostacyclin (iloprost, epoprostenol) | Some small case series suggest benefit; evidence insufficient for routine recommendation. Available on Authority PBS for other indications only. |
| Surgical embolectomy | Not feasible — emboli are diffuse and at the arteriolar level. Aortic endarterectomy carries further embolic risk. |
Long-Term Cardiovascular Risk Management
All patients with CES should receive aggressive secondary cardiovascular prevention:
- Statin therapy: high-intensity (atorvastatin 40–80 mg or rosuvastatin 20–40 mg daily) — lifelong.
- Antiplatelet therapy: aspirin 100 mg daily or clopidogrel 75 mg daily — lifelong (unless contraindicated).
- Blood pressure control: target <130/80 mmHg (or per individual renal tolerance).
- Smoking cessation: absolute priority — refer to Quitline (13 7848) and consider pharmacotherapy (varenicline PBS-listed).
- Diabetes optimisation: HbA1c target ≤53 mmol/mol (7.0 %) or individualised.
- Exercise and dietary counselling: cardiac rehabilitation programme if appropriate.
- Weight management: BMI <30 kg/m²; waist circumference targets.
Prognosis
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
📚 References
- 1. Scolari F, Ravani P. Atheroembolic renal disease. Lancet. 2010;375(9726):1650–1660.
- 2. Belenfant M, Meyrier A, Jacquot C. Supportive treatment improves survival in multivisceral cholesterol crystal embolism. Am J Kidney Dis. 1999;33(5):840–850.
- 3. Scolari F, Ravani P, Pola A, et al. Predictors of renal and patient outcomes in atheroembolic renal disease: a prospective study. J Am Soc Nephrol. 2003;14(6):1584–1590.
- 4. Modi KS, Rao VK. Atheroembolic renal disease. J Am Soc Nephrol. 2001;12(8):1781–1787.
- 5. Saric M, Kronzon I. Aortic atherosclerosis and embolic events. Curr Cardiol Rep. 2012;14(3):342–349.
- 6. Kronzon I, Saric M. Cholesterol embolization syndrome. Circulation. 2010;122(6):631–641.
- 7. Tayal R, Pollono E, Pahuja M, et al. Cholesterol embolization syndrome: a review of the current literature. J Invasive Cardiol. 2021;33(7):E530–E541.
- 8. The Royal Australian College of General Practitioners (RACGP). Guidelines for preventive activities in general practice. 10th edn. East Melbourne: RACGP; 2024.
- 9. Australian Institute of Health and Welfare (AIHW). Cardiovascular disease in Aboriginal and Torres Strait Islander people. Canberra: AIHW; 2023.
- 10. ANZDATA Registry. 46th Annual Report 2023. Adelaide: Australia and New Zealand Dialysis and Transplant Registry; 2023.
- 11. Heart Foundation of Australia. Absolute cardiovascular disease risk management. Melbourne: NHF; 2023.
- 12. RHDAustralia (ACIL Allen Consulting). The 2020 Australian guideline for prevention, diagnosis, and management of acute rheumatic fever and rheumatic heart disease. 3rd edn. Darwin: RHDAustralia; 2020.
- 13. Nair N, O'Driscoll J, Bhagat K. Cholesterol embolisation — an underdiagnosed cause of multisystem disease. BMJ. 2019;364:l586.
- 14. Australian Commission on Safety and Quality in Health Care (ACSQHC). National Safety and Quality Health Service Standards. 2nd edn. Sydney: ACSQHC; 2021.