📋 Key Information Summary
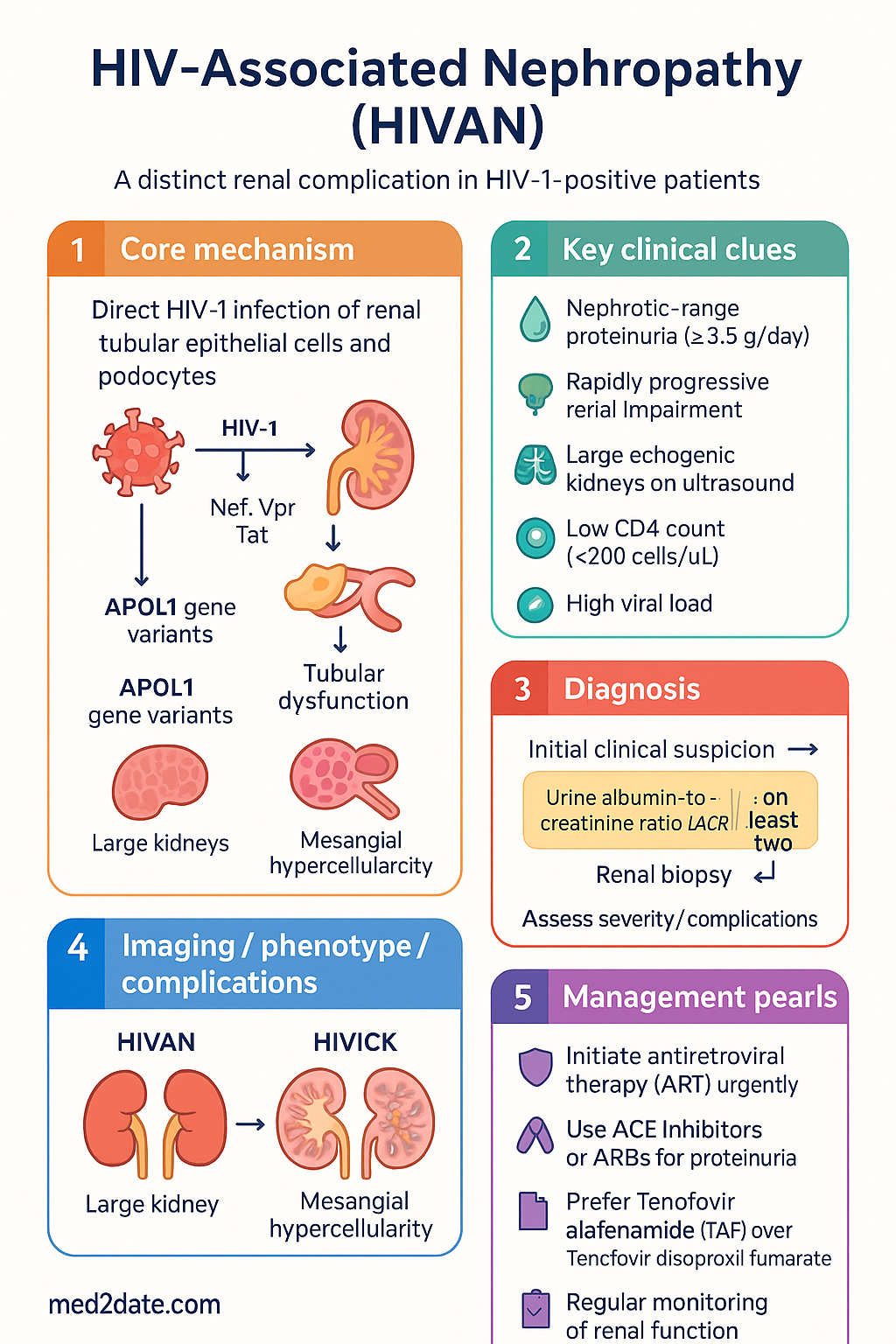
- HIV-associated nephropathy (HIVAN) is a collapsing variant of focal segmental glomerulosclerosis (FSGS) occurring in HIV-1-positive patients with low CD4 counts (<200 cells/µL) and high viral loads.
- HIVAN is the third leading cause of end-stage renal failure (ESRF) in African Americans aged 20–64; in Australia it remains an important differential in HIV-positive patients presenting with proteinuria or renal impairment.
- Direct HIV-1 infection of renal tubular epithelial cells and podocytes drives the pathogenesis via viral gene products (Nef, Vpr, Tat) causing dedifferentiation, proliferation, and apoptosis.
- Clinically presents with heavy proteinuria (often nephrotic-range >3.5 g/day), rapidly progressive renal impairment, and large echogenic kidneys on ultrasound.
- Renal biopsy is the gold standard — demonstrating collapsing glomerulopathy (collapsing FSGS), microcystic tubular dilatation, and interstitial inflammation.
- Antiretroviral therapy (ART) is the cornerstone of management — early initiation can halt or reverse renal injury and dramatically reduces ESRF risk.
- ACE inhibitors (ACEi) or angiotensin receptor blockers (ARB) are recommended to reduce proteinuria and slow disease progression, irrespective of blood pressure.
- Tenofovir disoproxil fumarate (TDF) carries nephrotoxic risk — tenofovir alafenamide (TAF) is preferred when available; monitor renal function if TDF is used.
- Corticosteroids (prednisolone) may be considered in severe or refractory cases, though evidence is limited and not from large RCTs.
- Aboriginal and Torres Strait Islander peoples have higher rates of HIV late diagnosis and concurrent renal disease — culturally safe, early screening is essential.
- All HIV-positive patients should have baseline and annual urine albumin-to-creatinine ratio (uACR) and eGFR monitoring.
- Referral to nephrology is recommended for all patients with suspected HIVAN for biopsy consideration and multidisciplinary care.
Introduction & Australian Epidemiology
HIV-associated nephropathy (HIVAN) is a distinct clinicopathological entity and the most common renal complication directly attributable to HIV-1 infection. It is characterised by a collapsing variant of focal segmental glomerulosclerosis (FSGS), microcystic tubular dilatation, and interstitial nephritis. HIVAN typically presents with heavy proteinuria and rapidly progressive renal impairment, and without treatment may progress to end-stage renal failure (ESRF) within weeks to months.
HIVAN was first described in 1984 among Black patients in the United States and remains overwhelmingly more prevalent in individuals of African descent, owing to genetic susceptibility variants in the APOL1 gene (G1 and G2 risk alleles). In Australia, HIVAN is an important but under-recognised diagnosis. The Kirby Institute reported approximately 29,045 people living with HIV in Australia as of 2022, with growing proportions of sub-Saharan African-born migrants and Aboriginal and Torres Strait Islander peoples — populations with higher background rates of renal disease and, in the case of African-born individuals, higher APOL1 risk allele prevalence.
In the pre-ART era, HIVAN accounted for up to 10–12% of ESRF in HIV-positive patients. Since the widespread adoption of combination ART, the incidence has declined substantially, but HIVAN persists — particularly among those with late HIV diagnosis, poor ART adherence, or advanced immunosuppression (CD4 <200 cells/µL). Australian data from tertiary renal units suggest HIVAN remains in the differential for collapsing FSGS, particularly in patients of African ancestry.
Pathophysiology — Direct HIV Infection of Podocytes
HIVAN is unique among HIV-related renal diseases because it results from direct infection of renal parenchymal cells by HIV-1, rather than from immune complex deposition or drug toxicity. The pathogenesis involves several key mechanisms:
Viral Entry & Tropism
HIV-1 infects renal tubular epithelial cells and, critically, glomerular podocytes. Unlike CD4+ T cells, renal cells lack the canonical CD4 receptor; viral entry occurs via alternative pathways including mannose receptors, galactosylceramide, and C-type lectins. Once integrated, HIV-1 proviral DNA persists within the renal epithelium, forming a renal reservoir independent of circulating viral load.
Viral Gene Products
- Nef: Expressed on podocyte surfaces, Nef activates Src kinase signalling (Src, Rac, STAT3), causing podocyte dedifferentiation, proliferation (a hallmark of collapsing FSGS), and loss of the mature podocyte phenotype (reduced synaptopodin, WT-1 expression).
- Vpr: A secreted protein that induces G2 cell-cycle arrest and apoptosis in tubular epithelial cells. Vpr is detectable in the urine of HIVAN patients and correlates with disease activity.
- Tat: Promotes tubular cell proliferation and fibrosis via upregulation of TGF-β and PDGF pathways.
- Gag/Pol: Contribute to endoplasmic reticulum stress and the unfolded protein response, driving tubular injury.
Host Genetic Susceptibility
Variants in the APOL1 gene (G1: rs73885319, rs60910145; G2: rs71785313) are the strongest host risk factors. Individuals carrying two APOL1 risk alleles have a 50-fold increased risk of HIVAN. These alleles are almost exclusive to individuals of recent African ancestry. In Australia, clinicians should consider APOL1 risk in patients of sub-Saharan African descent presenting with unexplained proteinuria in the setting of HIV.
Downstream Effects
Infected podocytes lose their differentiated phenotype and re-enter the cell cycle, leading to the characteristic collapsing glomerular tuft. Concurrently, microcystic tubular dilatation develops due to tubular epithelial proliferation and obstruction. Interstitial inflammation (CD8+ T-cell infiltrate) contributes to fibrosis and progressive renal scarring. The net result is rapid loss of nephron function, heavy proteinuria, and accelerated progression to ESRF.
Clinical Features & Diagnosis
Typical Presentation
HIVAN classically presents in patients with advanced HIV (CD4 <200 cells/µL, high viral loads, often ART-naïve). However, it may also occur in patients on suboptimal ART or with poor adherence. Key features include:
- Nephrotic-range proteinuria: Often >3.5 g/day; urine protein-to-creatinine ratio (uPCR) >350 mg/mmol.
- Rapidly progressive renal impairment: Creatinine may rise over days to weeks, mimicking acute kidney injury.
- Normal or low blood pressure: Unlike typical FSGS, hypertension is uncommon in HIVAN.
- Oedema and nephrotic syndrome: Peripheral oedema, hypoalbuminaemia, hypercholesterolaemia.
- Large, echogenic kidneys on ultrasound: Bilateral renal enlargement with increased cortical echogenicity — a useful bedside clue differentiating HIVAN from other causes of CKD where kidneys are typically small.
Diagnostic Criteria
There are no universally agreed clinical diagnostic criteria; however, HIVAN should be strongly suspected in an HIV-positive patient with:
- Proteinuria >1 g/day (or uPCR >100 mg/mmol) on at least two occasions
- Declining eGFR not attributable to prerenal, obstructive, or drug-related causes
- Large echogenic kidneys on renal ultrasound
- Absence of another glomerular disease (e.g., IgA nephropathy, lupus nephritis, diabetic nephropathy)
Differential Diagnosis of Renal Disease in HIV
| Condition | Key Features | Biopsy Finding |
|---|---|---|
| HIVAN (collapsing FSGS) | Nephrotic proteinuria, large kidneys, low CD4 | Collapsing FSGS, microcystic tubules |
| HIV immune complex kidney disease (HIVICK) | Variable proteinuria, may have haematuria | MPGN pattern, subendothelial deposits |
| IgA nephropathy | Visible haematuria, moderate proteinuria | Mesangial IgA deposits |
| Tenofovir nephrotoxicity | Proximal tubulopathy, declining eGFR | Proximal tubular injury, crystals |
| Thrombotic microangiopathy | AKI, microangiopathic haemolytic anaemia, thrombocytopenia | Thrombi in arterioles/glomeruli |
| Diabetic nephropathy | Long-standing DM, gradual proteinuria | Kimmelstiel–Wilson nodules, GBM thickening |
Investigations & Biopsy — Collapsing FSGS
Baseline Investigations
Renal Biopsy — Histopathological Features
The hallmark of HIVAN on renal biopsy is collapsing glomerulopathy, classified under the Columbia classification as a variant of FSGS. Key features include:
- Light microscopy: Collapse of glomerular capillary tufts with hypertrophy and hyperplasia of overlying podocytes (often with cytoplasmic vacuolisation). Microcystic dilatation of tubules is prominent. Interstitial inflammation with CD8+ T lymphocytes and mild fibrosis.
- Immunofluorescence: Typically negative or nonspecific (focal IgM, C3 in sclerotic segments). The absence of dominant immune complex deposits distinguishes HIVAN from HIVICK.
- Electron microscopy: Endothelial tubuloreticular inclusions (TRI) — pathognomonic structures within capillary endothelial cytoplasm, induced by interferon-α. Podocyte foot process effacement is widespread.
Risk Stratification
Risk factors for developing HIVAN and for progression to ESRF include:
Predictors of Poor Outcome
- Degree of interstitial fibrosis on biopsy (>40% fibrosis = poor prognosis)
- Presentation with ESRF requiring dialysis at diagnosis
- Failure to achieve viral suppression on ART
- Homozygous APOL1 G1/G2 risk alleles
- Coexistent hepatitis B or C co-infection
Management — ART & ACE Inhibitors
Antiretroviral Therapy (ART)
All patients with suspected or confirmed HIVAN should be on suppressive ART. Regimen selection should account for renal function and potential nephrotoxicity.
ACE Inhibitors & ARBs
ACE inhibitors (ACEi) or angiotensin receptor blockers (ARB) are recommended for all patients with HIVAN and proteinuria >1 g/day, regardless of blood pressure. They reduce intraglomerular pressure, proteinuria, and podocyte injury.
Corticosteroids
Corticosteroids may be considered in severe HIVAN (eGFR <30 or rapidly declining) that is not responding to ART optimisation within 2–4 weeks. Evidence is based on small cohort studies and case series; there are no large RCTs. Use only under specialist supervision.
Supportive Measures
- Sodium and fluid restriction: <2 g sodium/day if oedematous.
- Diuretics: Frusemide (Lasix®) 20–80 mg PO/IV daily for volume overload; add spironolactone if refractory (monitor K⁺).
- Statin therapy: Atorvastatin 10–40 mg PO daily for cardiovascular risk reduction (high CV burden in CKD + HIV). PBS General Benefit.
- Anticoagulation: Consider in nephrotic patients with serum albumin <20 g/L due to thrombotic risk (LMWH or warfarin).
- Vaccination: Ensure pneumococcal (Prevenar 13®, Pneumovax 23®), influenza, hepatitis B vaccination are up to date.
- Renal replacement therapy: Dialysis or transplant referral if progression to ESRF. HIV-positive patients can safely receive renal transplants with suppressed viral loads.
Management Timeline
Monitoring
Ongoing monitoring is essential in HIVAN to assess treatment response and detect complications:
| Parameter | Frequency | Target / Action |
|---|---|---|
| Serum creatinine / eGFR | Every 2–4 weeks (initially), then 3-monthly | Stabilisation or improvement; >5 mL/min decline → reassess ART, consider biopsy |
| uACR / uPCR | Monthly (initially), then 3-monthly | >50% reduction in proteinuria by 6 months is favourable |
| HIV viral load | At ART initiation, 4 weeks, 3 months, then 6-monthly | Undetectable (<20 copies/mL) by 6 months |
| CD4 count | Every 3–6 months | Recovery to >350 cells/µL; >500 is ideal |
| Serum potassium | 1–2 weeks after ACEi/ARB start/change, then 3-monthly | K⁺ <5.5 mmol/L; reduce/hold ACEi if hyperkalaemia |
| Serum phosphate, bicarbonate | 3-monthly if on TDF | Detect proximal tubulopathy (Fanconi syndrome) |
| Lipid panel | Baseline and annually | Statin if indicated for CV risk |
| Blood pressure | Every visit | Target <130/80 mmHg (KDIGO CKD guidelines) |
Special Populations
Aboriginal and Torres Strait Islander Health Considerations
Aboriginal and Torres Strait Islander peoples experience a disproportionate burden of both HIV and kidney disease in Australia. Late HIV diagnosis is more common, and concurrent risk factors for CKD — including diabetes, hypertension, and socioeconomic disadvantage — are prevalent. Culturally safe, community-led approaches to HIV testing and renal care are essential.
📚 References
- 1. Wyatt CM, Klotman PE, D'Agati VD. HIV-associated nephropathy: clinical presentation, pathology, and epidemiology in the era of antiretroviral therapy. Semin Nephrol. 2008;28(6):513–522.
- 2. Kopp JB, Nelson GW, Sampath K, et al. APOL1 genetic variants in focal segmental glomerulosclerosis and HIV-associated nephropathy. J Am Soc Nephrol. 2011;22(11):2129–2137.
- 3. Estrella M, Fine DM, Gallant JE, et al. HIV type 1 RNA level as a clinical indicator of renal disease in HIV-infected individuals. AIDS. 2007;21(3):355–360.
- 4. Lucas GM, Eustace JA, Sozio S, et al. Highly active antiretroviral therapy and the incidence of HIV-1-associated nephropathy: a 12-year cohort study. AIDS. 2004;18(3):541–546.
- 5. Rosenberg AZ, Naicker S, Winkler CA, Kopp JB. HIV-associated nephropathy: a review. Nephrol Dial Transplant. 2015;30(12):1991–1998.
- 6. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024;105(4S):S117–S314.
- 7. Australian Government Department of Health. Fifth National Aboriginal and Torres Strait Islander Blood-Borne Viruses and Sexually Transmissible Infections Strategy 2018–2022. Canberra: Commonwealth of Australia; 2018.
- 8. The Kirby Institute. HIV, viral hepatitis and sexually transmissible infections in Australia: Annual Surveillance Report 2023. Sydney: UNSW; 2023.
- 9. RACGP. National Guide to a Preventive Health Assessment for Aboriginal and Torres Strait Islander People. 4th edition. Melbourne: RACGP; 2018.
- 10. Australian Society for HIV, Viral Hepatitis and Sexual Health Medicine (ASHM). Antiretroviral Guidelines — Australian Commentary on the DHHS Guidelines. Sydney: ASHM; 2024.
- 11. Wearne N, Davidson B, Blockman M, Jones ESW, Dix-Peek T. HIV-associated nephropathy — a review of the current evidence. Curr Opin HIV AIDS. 2022;17(6):336–343.
- 12. Naicker S, Fabian J, Naidoo S, Muller E, Paget G, Cockburn I. Infection with human immunodeficiency virus (HIV) — end-stage renal disease: the experience in South Africa. J Ren Care. 2013;39(Suppl 1):3–9.
- 13. Campbell LJ, Ibrahim F, Fisher M, Holt SG, Post FA. Spectrum of chronic kidney disease in HIV-infected patients. HIV Med. 2009;10(6):329–336.
- 14. RHDAustralia (NACCHO & Menzies School of Health Research). Australian Guidelines for Sexual Health and Blood-borne Viruses — STI and BBV Management in Aboriginal and Torres Strait Islander Populations. Darwin: RHDAustralia; 2021.